
Even Grave Errors at Rehab Hospitals Go Unpenalized and Undisclosed
Rehab hospitals that help people recover from major surgeries and injuries have become a highly lucrative slice of the health care business.
But federal data and inspection reports show that some run by the dominant company, Encompass Health Corp., and other for-profit corporations have had rare but serious incidents of patient harm and perform below average on two key safety measures tracked by Medicare.
Yet even when inspections reveal grave cases of injury, federal health officials do not inform consumers or impose fines the way they do for nursing homes. And Medicare doesn’t provide easy-to-understand five-star ratings as it does for general hospitals.
In the most serious problems documented by regulators, rehab hospital errors involved patient deaths.
In Encompass Health’s hospital in Huntington, West Virginia, Elizabeth VanBibber, 73, was fatally poisoned by a carbon monoxide leak during construction at the facility.
At its hospital in Jackson, Tennessee, a patient, 68, was found dead overnight, lying on the floor in a “pool of blood” after an alarm that was supposed to alert nurses that he had gotten out of bed had been turned off.
In its hospital in Sioux Falls, South Dakota, a nurse gave Frederick Roufs, 73, the wrong drug, one of 26 medication errors the hospital made over six months. He died two days later at another hospital.
“I can still see Fred laying in the bed as they shut each little machine off,” said his widow, Susan Roufs. “They clicked four of them, and then the love of my life was gone.”
Encompass, which owns 168 hospitals and admitted 248,000 patients last year, has led the transformation of this niche industry. In 2023, stand-alone for-profit medical rehabilitation hospitals overtook nonprofits as the places where the majority of annual patient admissions occur, a KFF Health News and New York Times analysis found. A third of all admissions were to Encompass hospitals. Such facilities are required to provide three hours of therapy a day, five days a week.
Across the nation, there are now nearly 400 stand-alone rehab hospitals, the bulk of which are for-profit. These hospitals collectively generate profits of 10%, more than general hospitals, which earn about 6%, and far more than skilled nursing homes, which make less than 0.5%, according to the most recent data from the Medicare Payment Advisory Commission, an independent congressional agency.
At the same time, the number of small, specialized units within acute care hospitals — where most rehab used to be provided — has dwindled. There are now around 800 of those, and most are nonprofits.
In its latest annual report, Encompass, which is publicly traded, reported an 11% net profit in 2024, earning $597 million last year on revenues of $5.4 billion.
Federal data on the performance of about 1,100 of the rehab facilities show Encompass tends to be better at helping most patients return home and remain there. In a two-year period ending in September 2023, Medicare rated 233 rehab facilities as performing better than the national rate for this major metric, called “discharge to community.” Most rehabs with better community discharge rates are for-profit, and Encompass owns 79 of them.
But data from Medicare also reveals Encompass owns many of the rehabs with worse rates of potentially preventable, unplanned readmissions to general hospitals. Medicare evaluates how often patients are rehospitalized for conditions that might have been averted with proper care, including infections, bedsores, dehydration, and kidney failures.
Encompass accounts for about 1 in 7 rehab facilities nationally, but owned 34 of the 41 inpatient rehab facilities that Medicare rated as having statistically significantly worse rates of potentially preventable readmissions for discharged patients. (Overall, rates of readmission after discharge ranged from 7% to 12%, with a median of 9%.)
And it owned 28 of the 87 rehab facilities — 65 of which were for-profit — that had worse rates of potentially preventable readmissions to general hospitals during patient stays. (The median for these kinds of readmissions was 5%, and rates for individual rehabs ranged from 3% to 9%.)
Patrick Darby, the executive vice president and general counsel of Encompass, strongly defended the company’s record in written responses to questions. He dismissed Medicare’s readmissions ratings of “better,” “worse,” and “no different than the national rate” as “a crude scoring measure” and said “performance is so similar across the board.” He called the violations found during health inspections “rare occurrences” that “do not support an inference of widespread quality concerns.”
“The simplest and most accurate reason for EHC’s success is that our hospitals provide superior care to patients,” he said, referring to Encompass by its corporate initials.
Chih-Ying Li, an associate professor of occupational therapy at the University of Texas Medical Branch at Galveston School of Health Professions, said in an interview that a research study she conducted found the profit status of a rehab facility was the only characteristic associated with higher unplanned readmissions.
“The finding is pretty robust,” she said. “It’s not like huge, huge differences, but there are differences.”
VanBibber was admitted to Encompass’ Huntington hospital in 2021 for therapy to strengthen her lungs. At the time, the hospital was undergoing a $3 million expansion, and state regulators had warned the company that areas of the hospital occupied by patients had to be isolated from the construction “using airtight barriers,” according to a health inspection report.
In her room, which was about 66 feet from the construction zone, she began having trouble breathing, the report said. When she told the staff, they ignored her and shut her door, according to a lawsuit brought by her estate. Staff members eventually noticed that she was “lethargic and gasping for air,” and called 911.
When the emergency medical squad arrived, the carbon monoxide detectors they wore sounded. By that time, VanBibber’s blood oxygen levels were dangerously low, the inspection report said. She died three days later from respiratory failure and carbon monoxide poisoning, according to the inspection report and the lawsuit. A plumber had been using a gas-powered saw in the construction area, but there were no carbon monoxide detectors in the hallways, the report said.
In court papers, Encompass and its construction contractors denied negligence for VanBibber’s death. The case is pending.
Inspectors determined Encompass failed to maintain a safe environment for all patients during construction and didn’t properly evaluate other patients for signs of poisoning, the report said.
Since 2021, the federal Centers for Medicare and Medicaid Services, or CMS, which oversees health inspections, has found that 10 Encompass hospitals, including the one that cared for VanBibber, had immediate jeopardy violations, federal records show. Such violations — like the ones that Medicare also found in connection with the deaths of Roufs and the patient who fell after leaving his bed — mean a hospital’s failure to comply with federal rules has put patients at risk for serious injury, serious harm, serious impairment, or death.
Darby, the general counsel for Encompass, said the company regretted any clinical problems and had promptly addressed all such findings to the satisfaction of inspectors. He said Encompass that has an “excellent compliance record,” including superior results from its accreditation agency, and that its overall number of health citations was tiny given how many hospitals Encompass owns and how many patients it treats.
Six other corporate-operated for-profit hospitals were also cited, while none of the 31 stand-alone nonprofit rehab hospitals received such violations from 2021 to 2024. (Inspection reports for general hospitals do not systematically specify in which part of the building a violation occurred, so rehab unit violations cannot be identified.)
An alert called a bed alarm was at the root of immediate jeopardies at Encompass hospitals in Morgantown, West Virginia, and Jackson, Tennessee. The devices are pressure- and motion-sensitive and emit a sound and display a light to alert staff members that someone at a high risk of falls has left his or her bed.
In its Morgantown hospital, a nurse technician discovered a patient face down on the floor with a large gash on her head after a defective alarm did not go off, an inspection report said. After she died, the nurse told inspectors: “We are having a lot of problems with the bed alarms.”
Medicare is not authorized by law to fine rehab hospitals for safety rule violations, even ones involving deaths uncovered during inspections, as it has done with nearly 8,000 nursing homes during the last three years, imposing average fines of about $28,000.
The only option is to entirely cut off a rehab hospital’s reimbursement for all services by Medicare and Medicaid, which cover most patients. That step would most likely put it out of business and is almost never used because of its draconian consequences.
“Termination is typically a last resort after working with the provider to come back into compliance,” Catherine Howden, a CMS spokesperson, said in an email.
As a result, because there’s no graduated penalty, even the most serious — and rare — immediate jeopardy violations effectively carry no punishments so long as the hospital puts steps in place to avert future problems.
“Only having a nuclear weapon has really hurt patient safety,” said Michael Millenson, a medical quality advocate.
One immediate jeopardy incident did result in a punishment, but only because the hospital was in California, which allows its health department to issue penalties. Encompass’ Bakersfield hospital paid a $75,000 fine last year for failing to control the blood sugar of a patient who died after her heart stopped.
Rapid Growth and a Troubled History
Encompass has accelerated its expansion in recent years and now operates in 38 states and Puerto Rico. It plans to open 17 more hospitals in Arizona, Connecticut, Florida, Georgia, Maine, Pennsylvania, South Carolina, Texas, and Utah by the end of 2027, according to its latest report.
It frequently moves into new markets by persuading local nonprofit hospitals to shutter their rehab units in exchange for an equity stake in a newly built Encompass hospital, company executives have told investors.
The president of Encompass, Mark Tarr, calls it a “win-win proposition”: The local hospitals can use their emptied space for a more lucrative line of service and Encompass gets a “jump start” into a new market, with partner hospitals often referring patients.
Tarr, who was paid $9.3 million in compensation last year, told investors that Encompass requires that the existing hospitals sign a noncompete deal. Sixty-seven Encompass hospitals are joint ventures, mostly with nonprofit hospitals as investors, according to the company’s June financial filing, the most recent available.
Darby said the company’s profits allow it to build hospitals in areas that lack intensive inpatient rehabilitation and improve existing hospitals. “High-quality patient care is not only consistent with shareholder return, but quality and shareholder return are in fact critical to one another,” he said.
The success of Encompass is particularly notable given that it barely survived what experts said was one of the largest modern accounting scandals in 2003.
The Securities and Exchange Commission charged that the company, then known as HealthSouth, overstated earnings by $2.7 billion to meet Wall Street analyst quarterly expectations, leading to the ouster of its founder and directors. In 2004, the company agreed to pay the government $325 million to settle Medicare fraud allegations without admitting wrongdoing. Darby credited the company’s new leaders for obtaining a $2.9 billion judgment on behalf of shareholders against the company’s founder.
The company changed its name to Encompass in 2018 after acquiring Encompass Home Health and Hospice. In 2019, the Justice Department announced the company had agreed to pay $48 million to settle whistleblower lawsuit claims that it misdiagnosed patients to get higher Medicare reimbursements, and admitted patients who were too sick to benefit from therapy. The company denied any wrongdoing, blaming independent physicians who worked at its hospitals. Darby said Encompass settled the case only to “avoid more years of expense and disruption.” He said the Justice Department never filed a lawsuit despite years of investigation.
Medication Harms
Rehab hospital inspection reports are not posted on Care Compare, Medicare’s online search tool for consumers. KFF Health News had to sue CMS under the Freedom of Information Act to obtain all its inspection reports for rehab hospitals. In contrast, Care Compare publishes all nursing home inspection reports and assigns each facility a star rating for its adherence to health and safety rules.
So people now choosing a rehab hospital would not know that at the Encompass hospital in Sioux Falls, South Dakota, in 2021, a nurse accidentally gave Roufs a blood pressure drug called hydralazine instead of hydroxyzine, his prescribed anti-anxiety medication, according to an inspection report. Roufs went into cardiac arrest. This type of error, called a “look-alike/sound-alike,” is one hospitals and staff members are supposed to be especially alert to.
Months before, an internal safety committee had identified a trend of medication errors, including when a nurse accidentally gave a patient 10 times the prescribed amount of insulin, sending him to the hospital, the inspection report said. The nurse had misread four units as 40. Since Roufs’s death, inspectors have faulted the hospital six times for various lapses, most recently in April 2024 for improper wound care.
An Encompass hospital in Texarkana, Texas, misused antipsychotic medications to pacify patients, resulting in an immediate jeopardy finding from CMS, the report said. And the company’s hospital in Erie, Pennsylvania, was issued an immediate jeopardy violation for not keeping track of medication orders in 2023, when a patient had a cardiac arrest after not receiving all of his drugs, according to the inspection report.
The federal government’s overall quality oversight efforts are limited. Medicare docks payment to rehab facilities for patients readmitted to a general hospital during shorter-than-average rehab stays, but unlike at general hospitals, there are no financial penalties when recently discharged rehab patients are hospitalized for critical health issues.
The Biden administration announced last year it intended to develop a rating scale of 1 to 5 stars for rehab facilities. The industry’s trade association, the American Medical Rehabilitation Providers Association, requested a delay in the creation of star ratings until the current quality measures were refined. The Trump administration has not determined whether it will continue the effort to rate rehab facilities, according to a CMS spokesperson.
Deadly Bedsores
The family of Paul Webb Jr., 74, claimed in a lawsuit that the Encompass hospital in Erie left Webb unattended in a wheelchair for hours at a time, putting pressure on his tailbone, in 2021. His medical records, provided to reporters by the family, list a sitting tolerance of one hour.
Webb — who had been originally hospitalized after a brain bleed, a type of stroke — developed skin damage known as a pressure sore, or bedsore, on his bottom, the lawsuit said. The suit said the sore worsened after he was sent to a nursing home, which the family is also suing, then home, and he died later that year. In his final weeks, Webb was unable to stand, sit, or move much because of the injury, the lawsuit said.
In court papers, Encompass and the nursing home denied negligence, as Encompass has in some other pending and closed lawsuits that accused it of failing to prevent pressure sores because nurses and aides failed to regularly reposition patients, or notice and treat emerging sores. Darby said Webb’s death occurred three months after his Encompass stay and was not related to his care at Encompass. He said no hospital with long-term patients could prevent every new or worsening pressure sore, but that Encompass’ rates were similar to the 1% national average.
One of Webb’s sons, Darel Webb, recalled a warning given to the family as they left an appointment their father had with wound specialists: A doctor brought up Christopher Reeve, the actor who played Superman in movies in the 1970s and 1980s.
“He goes, ‘Remember, Superman was paralyzed from falling off the horse, but he died from a bedsore,’” he said.
Jordan Rau has been writing about hospital safety since 2008. Irena Hwang is a New York Times data reporter who uses computational tools to uncover hidden stories and illuminate the news.
METHODOLOGY
To examine the medical rehabilitation hospital industry, we obtained and analyzed a database of inspection reports of freestanding rehabilitation hospitals from the federal Centers for Medicare & Medicaid Services, or CMS. We also obtained inspection reports from several states through public records requests.
We analyzed inpatient rehabilitation facility characteristics and patient volume data contained in hospital data files from the Rand Corp., a nonprofit research organization. This dataset compiles cost reports all hospitals submit each year to CMS. For each facility for the years 2012 to 2023, we categorized annual discharges by facility type (freestanding rehabilitation hospital or unit within an acute care hospital); facility ownership status (for-profit, nonprofit, or government); and which hospitals were owned by Encompass Health under its current or prior name, HealthSouth.
Financial information about Encompass Health was obtained from the company’s Securities and Exchange Commission disclosure filings.
We examined the readmission rates for all inpatient rehabilitation facilities that CMS publishes in its quality data. CMS evaluates the frequency with which Medicare patients were readmitted for potentially preventable reasons to an acute care hospital during their rehab stay. Separately, CMS also evaluates the frequency of potentially preventable readmissions to an acute care hospital within 30 days of discharge from rehab. We also examined the rate of successful return to home or community. Figures for all three metrics were available for about 1,100 of the roughly 1,200 rehab facilities in the CMS data. The most recent readmission data covered Medicare discharges from October 2021 through September 2023.
We examined nursing home penalties from the last three years from CMS’ data on nursing homes.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
1 week 1 day ago
Health Industry, Insurance, Medicare, Multimedia, Arizona, california, CMS, Connecticut, Florida, Georgia, Hospitals, Investigation, Maine, New York, Pennsylvania, South Carolina, South Dakota, Tennessee, texas, Utah, West Virginia

As Mosquito Season Peaks, Officials Brace for New Normal of Dengue Cases
As summer ushers in peak mosquito season, health and vector control officials are bracing for the possibility of another year of historic rates of dengue.
As summer ushers in peak mosquito season, health and vector control officials are bracing for the possibility of another year of historic rates of dengue. And with climate change, the lack of an effective vaccine, and federal research cuts, they worry the disease will become endemic to a larger swath of North America.
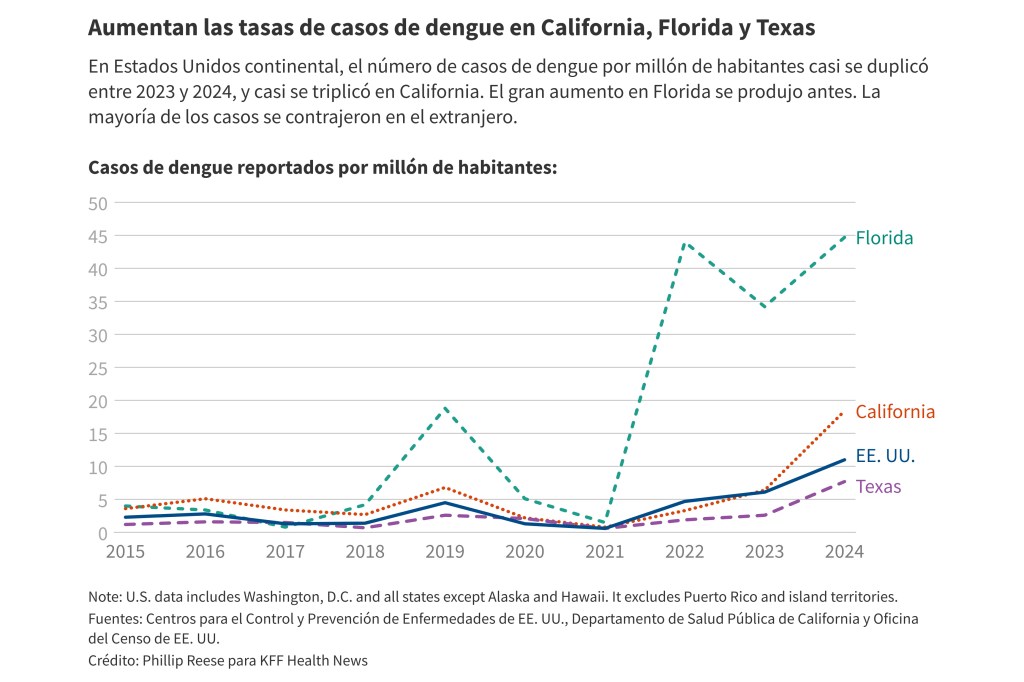
About 3,700 new dengue infections were reported last year in the contiguous United States, up from about 2,050 in 2023, according to the Centers for Disease Control and Prevention. All of last year’s cases were acquired abroad, except for 105 cases contracted in California, Florida, or Texas. The CDC issued a health alert in March warning of the ongoing risk of dengue infection.
“I think dengue is here with us to stay,” said infectious disease specialist Michael Ben-Aderet, associate medical director of hospital epidemiology at Cedars-Sinai in Los Angeles, about dengue becoming a new normal in the U.S. “These mosquitoes aren't going anywhere.”
Dengue is endemic — a label health officials assign when diseases appear consistently in a region — in many warmer parts of the world, including Latin America, India, and Southeast Asia. Dengue cases increased markedly last year in many of those places, especially in Central and South America.
The disease, which can spread when people are bitten by infected Aedes mosquitoes, was not common in the contiguous United States for much of the last century. Today, most locally acquired (meaning unrelated to travel) dengue cases in the U.S. happen in Puerto Rico, which saw a sharp increase in 2024, triggering a local public health emergency.
Most people who contract dengue don’t get sick. But in some people symptoms are severe: bleeding from the nose or mouth, intense stomach pain, vomiting, and swelling. Occasionally, dengue causes death.
California offers a case study in how dengue is spreading in the U.S. The Aedes aegypti and Aedes albopictus mosquitoes that transmit dengue weren’t known to be in the state 25 years ago. They are now found in 25 counties and more than 400 cities and unincorporated communities, mostly in Southern California and the Central Valley.
The spread of the mosquitoes is concerning because their presence increases the likelihood of disease transmission, said Steve Abshier, president of the Mosquito and Vector Control Association of California.
From 2016 through 2022, there were an average of 136 new dengue cases a year in California, each case most likely brought to the state by someone who had traveled and been infected elsewhere. In 2023, there were about 250 new cases, including two acquired locally.
In 2024, California saw 725 new dengue cases, including 18 acquired locally, state data shows.
Climate change could contribute to growth in the Aedes mosquitoes’ population, Ben-Aderet said. These mosquitoes survive best in warm urban areas, often biting during the daytime. Locally acquired infections often occur when someone catches dengue during travel, then comes home and is bitten by an Aedes mosquito that bites and infects another person.
“They've just been spreading like wildfire throughout California,” Ben-Aderet said.
Dengue presents a challenge to the many primary care doctors who have never seen it. Ben-Aderet said doctors who suspect dengue should obtain a detailed travel history from their patients, but confirming the diagnosis is not always quick.
“There's no easy test for it,” he said. “The only test that we have for dengue is antibody tests.” He added that “most labs probably aren't doing it commercially, so it's usually like a send-out test from most labs. So you really have to suspect someone has dengue.”
Best practices for avoiding dengue include eliminating any standing pools of water on a property — even small pools — and using mosquito repellent, Abshier said. Limiting activity at dusk and dawn, when mosquitoes bite most often, can also help.
Efforts to combat dengue in California became even more complicated this year after wildfires ripped through Los Angeles. The fires occurred in a hot spot for mosquito-borne illnesses. San Gabriel Valley Mosquito and Vector Control District officials have worked for months to treat more than 1,400 unmaintained swimming pools left in the wake of fire, removing potential breeding grounds for mosquitoes.
San Gabriel vector control officials have used local and state resources to treat the pools, said district spokesperson Anais Medina Diaz. They have applied for reimbursement from the Federal Emergency Management Agency, which has not historically paid for vector control efforts following wildfires.
In California, vector control agencies are often primarily funded by local taxes and fees on property owners.
Some officials are pursuing the novel method of releasing sterilized Aedes mosquitoes to reduce the problem. That may prove effective, but deploying the method in a large number of areas would be costly and would require a massive effort at the state level, Abshier said. Meanwhile, the federal government is pulling back on interventions: Several outlets have reported that the National Institutes of Health will stop funding new climate change-related research, which could include work on dengue.
This year, reported rates of dengue in much of the Americas have declined significantly from 2024. But the trend in the United States likely won’t be clear until later in the year, after the summer mosquito season ends.
Health and vector control researchers aren't sure how bad it will get in California. Some say there may be limited outbreaks, while others predict dengue could get much worse. Sujan Shresta, a professor and infectious disease researcher at the La Jolla Institute for Immunology, said other places, like Nepal, experienced relatively few cases of dengue in the recent past but now regularly see large outbreaks.
There is a vaccine for children, but it faces discontinuation from a lack of global demand. Two other dengue vaccines are unavailable in the United States. Shresta’s lab is hard at work on an effective, safe vaccine for dengue. She hopes to release results from animal testing in a year or so; if the results are positive, human trials could be possible in about two years.
“If there's no good vaccine, no good antivirals, this will be a dengue-endemic country,” she said.
Phillip Reese is a data reporting specialist and an associate professor of journalism at California State University-Sacramento.
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 weeks 22 hours ago
california, Multimedia, Public Health, States, Environmental Health, Florida, texas
Con el verano hay más mosquitos y, temen oficiales, más casos de dengue
Con el verano marcando el comienzo de la temporada alta de mosquitos, autoridades sanitarias y de control de vectores se preparan para la posibilidad de otro año con tasas históricas de dengue.
Con el verano marcando el comienzo de la temporada alta de mosquitos, autoridades sanitarias y de control de vectores se preparan para la posibilidad de otro año con tasas históricas de dengue. Y con el cambio climático, la falta de una vacuna eficaz y los recortes federales en la investigación, les preocupa que la enfermedad se vuelva endémica en una franja más amplia de Norteamérica.
El año pasado se reportaron alrededor de 3.700 nuevas infecciones por dengue en Estados Unidos, frente a las 2.050 de 2023, según los Centros para el Control y Prevención de Enfermedades (CDC). Todos los casos de 2024 se adquirieron en el extranjero, excepto 105 contraídos en California, Florida o Texas. Los CDC emitieron una alerta sanitaria en marzo advirtiendo sobre el riesgo continuo de infección por dengue.
"Creo que el dengue ha llegado para quedarse", declaró Michael Ben-Aderet, especialista en enfermedades infecciosas y director médico asociado de epidemiología hospitalaria del Cedars-Sinai de Los Ángeles, sobre la posibilidad de que el dengue se convierta en la nueva normalidad en el país. "Estos mosquitos no se irán a ninguna parte".
El dengue es endémico —una etiqueta que las autoridades de salud pública asignan cuando las enfermedades aparecen de forma constante en una región— en muchas zonas más cálidas del mundo, como Latinoamérica, India y el sudeste asiático. Los casos de dengue aumentaron notablemente el año pasado en muchos de esos lugares, especialmente en Centro y Sur América.
La enfermedad, que puede propagarse por la picadura de mosquitos Aedes que portan el virus, no fue común en Estados Unidos continental durante gran parte del siglo pasado. Actualmente, la mayoría de los casos de dengue adquiridos localmente (es decir, no relacionados con viajes) en el país se registran en Puerto Rico, donde se registró un fuerte aumento en 2024, lo que desencadenó una emergencia de salud pública local.
La mayoría de las personas que desarrollan dengue no se enferman. Sin embargo, en algunas, los síntomas son graves: sangrado por la nariz o la boca, dolor de estómago intenso, vómitos e hinchazón. En ocasiones, el dengue causa la muerte.
California ofrece un caso centinela sobre la propagación del dengue en el país. Hace 25 años, no se conocía la presencia de los mosquitos Aedes aegypti y Aedes albopictus, que transmiten el dengue, en el estado. Actualmente, se encuentran en 25 condados y más de 400 ciudades y comunidades no incorporadas, principalmente en el sur de California y en el Valle Central.
La propagación de los mosquitos es preocupante porque su presencia aumenta la probabilidad de transmisión de enfermedades, afirmó Steve Abshier, presidente de la Mosquito and Vector Control Association of California.
Entre 2016 y 2022, se registró un promedio de 136 nuevos casos de dengue al año en California, cada uno de los cuales probablemente traído al estado por alguien que viajó y se infectó en otro lugar. En 2023, se registraron alrededor de 250 casos nuevos, incluyendo dos adquiridos localmente.
En 2024, California registró 725 nuevos casos de dengue, incluyendo 18 adquiridos localmente, según datos estatales.
El cambio climático podría contribuir al aumento de la población de mosquitos Aedes, afirmó Ben-Aderet. Estos mosquitos sobreviven mejor en zonas urbanas cálidas, y suelen picar durante el día. Las infecciones de transmisión local suelen ocurrir cuando alguien contrae dengue durante un viaje, regresa a casa y lo pica un mosquito Aedes que, a su vez, pica e infecta a otra persona.
"Se han propagado rápidamente por toda California", explicó Ben-Aderet.
El dengue representa un desafío para muchos médicos de atención primaria que nunca lo han visto. Ben-Aderet dijo que los médicos que sospechan dengue deben obtener un historial de viaje detallado de sus pacientes, pero confirmar el diagnóstico no siempre es rápido.
"No existe una prueba sencilla para detectarlo", afirmó. "La única prueba que tenemos para el dengue son las pruebas de anticuerpos". Agregó que "la mayoría de los laboratorios probablemente no lo estén comercializando, por lo que suele ser una prueba que se debe analizar en otra instalación. Por lo tanto, es fundamental sospechar que alguien tiene dengue".
Las mejores prácticas para evitar el dengue incluyen eliminar cualquier agua estancada en una propiedad, aunque sea poca, y usar repelente de mosquitos, dijo Abshier. Limitar la actividad al atardecer y al amanecer, cuando los mosquitos pican con mayor frecuencia, también puede ayudar.
Los esfuerzos para combatir el dengue en California se complicaron aún más este año después de que los incendios forestales arrasaran Los Ángeles.
Los incendios ocurrieron en una zona de alta incidencia de enfermedades transmitidas por mosquitos. Funcionarios del San Gabriel Valley Mosquito and Vector Control District han trabajado durante meses para tratar más de 1.400 piscinas sin mantenimiento que quedaron tras el incendio, eliminando así posibles criaderos de mosquitos.
Estos oficiales han utilizado recursos locales y estatales para tratar las piscinas, dijo Anais Medina Díaz, vocera del distrito. Han solicitado un reembolso a la Agencia Federal para el Manejo de Emergencias (FEMA), que históricamente no ha financiado las iniciativas de control de vectores luego de incendios forestales.
En California, las agencias de control de vectores suelen financiarse principalmente con impuestos y tasas locales que pagan los propietarios.
Algunos funcionarios están implementando el novedoso método de liberar mosquitos Aedes esterilizados para reducir el problema. Eso puede resultar eficaz, pero implementar el método en un gran número de áreas sería costoso y requeriría un esfuerzo masivo a nivel estatal, dijo Abshier.
Mientras tanto, el gobierno federal está reduciendo sus intervenciones: varios medios han informado que los Institutos Nacionales de Salud dejarán de financiar nuevas investigaciones relacionadas con el cambio climático, que podrían incluir trabajos sobre el dengue.
Este año, las tasas de dengue reportadas en gran parte del continente americano han disminuido significativamente desde 2024. Sin embargo, es probable que la tendencia en Estados Unidos no se esclarezca hasta finales de año, después que termine la temporada de mosquitos de verano.
Los investigadores de salud y control de vectores no están seguros de la gravedad de la situación en California.
Algunos afirman que podría haber brotes limitados, mientras que otros predicen que el dengue podría empeorar mucho. Sujan Shresta, profesor e investigador de enfermedades infecciosas en el Instituto de Inmunología de La Jolla, señaló que otros lugares, como Nepal, experimentaron relativamente pocos casos de dengue en el pasado reciente, pero ahora se registran brotes grandes con regularidad.
Existe una vacuna para niños, pero está siendo discontinuada debido a la falta de demanda mundial. Otras dos vacunas no están disponibles en Estados Unidos. El laboratorio de Shresta trabaja arduamente en una vacuna eficaz y segura contra el dengue. Espera publicar los resultados de las pruebas en animales en aproximadamente un año; si son positivos, los ensayos en humanos podrían ser posibles en unos dos años.
"Si no hay una buena vacuna ni buenos antivirales, este será un país endémico para dengue", afirmó.
Phillip Reese es especialista en reportaje de datos y profesor asociado de Periodismo en la Universidad Estatal de California-Sacramento.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 weeks 22 hours ago
Global Health Watch, Noticias En Español, Public Health, States, california, Florida, Latinos, texas

In a Dusty Corner of California, Trump’s Threatened Cuts to Asthma Care Raise Fears
Esther Bejarano’s son was 11 months old when asthma landed him in the hospital. She didn’t know what had triggered his symptoms — neither she nor her husband had asthma — but she suspected it was the pesticides sprayed on the agricultural fields near her family’s home.
Pesticides are a known contributor to asthma and are commonly used where Bejarano lives in California’s Imperial Valley, a landlocked region that straddles two counties on the U.S.-Mexico border and is one of the main producers of the nation’s winter crops. It also has some of the worst air pollution in the nation and one of the highest rates of childhood asthma emergency room visits in the state, according to data collected by the California Department of Public Health.
Bejarano has since learned to manage her now-19-year-old son’s asthma and works at Comite Civico del Valle, a local rights organization focused on environmental justice in the Imperial Valley. The organization trains health care workers to educate patients on proper asthma management, enabling them to avoid hospitalization and eliminate triggers at home. The course is so popular that there’s a waiting list, Bejarano said.
But the group’s Asthma Management Academy program and similar initiatives nationwide face extinction with the Trump administration’s mass layoffs, grant cancellations, and proposed budget cuts at the Department of Health and Human Services and the Environmental Protection Agency. Asthma experts fear the cumulative impact of the reductions could result in more ER visits and deaths, particularly for children and people in low-income communities — populations disproportionately vulnerable to the disease.
“Asthma is a preventive condition,” Bejarano said. “No one should die of asthma.”
Asthma can block airways, making it hard to breathe, and in severe cases can cause death if not treated quickly. Nearly 28 million people in the U.S. have asthma, and about 10 people still die every day from the disease, according to the Asthma and Allergy Foundation of America.
In May, the White House released a budget proposal that would permanently shutter the Centers for Disease Control and Prevention’s National Asthma Control Program, which was already gutted by federal health department layoffs in April. It’s unclear whether Congress will approve the closure.
Last year, the program allotted $33.5 million to state-administered initiatives in 27 states, Puerto Rico, and Washington, D.C., to help communities with asthma education. The funding is distributed in four-year grant cycles, during which the programs receive up to $725,000 each annually.
Comite Civico del Valle’s academy in Southern California, a clinician workshop in Houston, and asthma medical management training in Allentown, Pennsylvania — ranked the most challenging U.S. city to live in with asthma — are among the programs largely surviving on these grants. The first year of the current grant cycle ends Aug. 31, and it’s unknown whether funding will continue beyond then.
Data suggests that the CDC’s National Asthma Control Program has had a significant impact. The agency’s own research has shown that the program saves $71 in health care costs for every $1 invested. And the asthma death rate decreased 44% between the 1999 launch of the program and 2021, according to the American Lung Association.
“Losing support from the CDC will have devastating impacts on asthma programs in states and communities across the country, programs that we know are improving the lives of millions of people with asthma,” said Anne Kelsey Lamb, director of the Public Health Institute’s Regional Asthma Management and Prevention program. “And the thing is that we know a lot about what works to help people keep their asthma well controlled, and that’s why it’s so devastating.”
The Trump administration cited cost savings and efficiency in its April announcement of the cuts to HHS. Requests for comment from the White House and CDC about cuts to federal asthma and related programs were not answered.
The Information Wars
Fresno, in the heart of California’s Central Valley, is one of the country’s top 20 “asthma capitals,” with high rates of asthma and related emergencies and deaths. It’s home to programs that receive funding through the National Asthma Control Program. Health care professionals there also rely on another aspect of the program that is under threat if it’s shuttered: countrywide data.
The federal asthma program collects information on asthma rates and offers a tool to study prevalence and rates of death from the disease, see what populations are most affected, and assess state and local trends. Asthma educators and health care providers worry that the loss of these numbers could be the biggest impact of the cuts, because it would mean a dearth of information crucial to forming educated recommendations and treatment plans.
“How do we justify the services we provide if the data isn’t there?” said Graciela Anaya, director of community health at the Central California Asthma Collaborative in Fresno.
Mitchell Grayson, chair of the Asthma and Allergy Foundation’s Medical Scientific Council, is similarly concerned.
“My fear is we’re going to live in a world that is frozen in Jan. 19, 2025, as far as data, because that was the last time you know that this information was safely collected,” he said.
Grayson, an allergist who practices in Columbus, Ohio, said he also worries government websites will delete important recommendations that asthma sufferers avoid heavy air pollution, get annual flu shots, and get covid-19 vaccines.
Disproportionate Risk
Asthma disproportionately affects communities of color because of “historic structural issues,” said Lynda Mitchell, CEO of the Asthma and Allergy Network, citing a higher likelihood of living in public housing or near highways and other pollution sources.
She and other experts in the field said cuts to diversity initiatives across federal agencies, combined with the rollback of environmental protections, will have an outsize impact on these at-risk populations.
In December, the Biden administration awarded nearly $1.6 billion through the EPA’s Community Change Grants program to help disadvantaged communities address pollution and climate threats. The Trump administration moved to cut this funding in March. The grant freezes, which have been temporarily blocked by the courts, are part of a broader effort by the Trump EPA to eliminate aid to environmental justice programs across the agency.
In 2023 and 2024, the National Institutes of Health’s Climate Change and Health Initiative received $40 million for research, including on the link between asthma and climate change. The Trump administration has moved to cut that money. And a March memo essentially halted all NIH grants focused on diversity, equity, and inclusion, or DEI — funds many of the asthma programs serving low-income communities rely on to operate.
On top of those cuts, environmental advocates like Isabel González Whitaker of Memphis, Tennessee, worry that the proposed reversals of environmental regulations will further harm the health of communities like hers that are already reeling from the effects of climate change. Shelby County, home to Memphis, recently received an “F” on the American Lung Association’s annual report card for having so many high ozone days. González Whitaker is director of EcoMadres, a program within the national organization Moms for Clean Air that advocates for better environmental conditions for Latino communities.
“Urgent asthma needs in communities are getting defunded at a time when I just see things getting worse in terms of deregulation,” said González Whitaker, who took her 12-year-old son to the hospital because of breathing issues for the first time this year. “We’re being assaulted by this data and science, which is clearly stating that we need to be doing better around preserving the regulations.”
Back in California’s Imperial Valley — where the majority-Hispanic, working-class population surrounds California’s largest lake, the Salton Sea — is an area called Bombay Beach. Bejarano calls it the “forgotten community.” Homes there lack clean running water, because of naturally occurring arsenic in the groundwater, and residents frequently experience a smell like rotten eggs blowing off the drying lakebed, exposing decades of pesticide-tinged dirt.
In 2022, a 12-year-old girl died in Bombay Beach after an asthma attack. Bejarano said she later learned that the girl’s school had recommended that she take part in Comite Civico del Valle’s at-home asthma education program. She said the girl was on the waiting list when she died.
“It hit home. Her death showed the personal need we have here in Imperial County,” Bejarano said. “Deaths are preventable. Asthma is reversible. If you have asthma, you should be able to live a healthy life.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
1 month 2 weeks ago
california, Public Health, Rural Health, States, Children's Health, HHS, Pennsylvania, Tennessee, texas, Trump Administration

KFF Health News' 'What the Health?': Bill With Billions in Health Program Cuts Passes House
The Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
With only a single vote to spare, the House passed a controversial budget bill that includes billions of dollars in tax cuts for the wealthy, along with billions of dollars of cuts to Medicaid, the Affordable Care Act, and the food stamp program — most of which will affect those at the lower end of the income scale. But the bill faces an uncertain future in the Senate.
Meanwhile, Health and Human Services Secretary Robert F. Kennedy Jr. released a report from his commission to “Make America Healthy Again” that described threats to the health of the American public — but notably included nothing on threats from tobacco, gun violence, or a lack of health insurance.
This week’s panelists are Julie Rovner of KFF Health News, Anna Edney of Bloomberg News, Sarah Karlin-Smith of the Pink Sheet, and Alice Miranda Ollstein of Politico.
Panelists
Anna Edney
Bloomberg News
Sarah Karlin-Smith
Pink Sheet
@sarahkarlin-smith.bsky.social
Alice Miranda Ollstein
Politico
Among the takeaways from this week’s episode:
- House Republicans passed their “big, beautiful” bill 215-214 this week, with one Republican critic voting present. But the Senate may have its own “big, beautiful” rewrite. Some conservative senators who worry about federal debt are concerned that the bill is not fully paid for and would add to the budget deficit. Others, including some red-state Republicans, say the bill’s cuts to Medicaid and food assistance go too far and would hurt low-income Americans. The bill’s cuts would represent the biggest reductions to Medicaid in the program’s 60-year history.
- Many of the bill’s Medicaid cuts would come from adding work requirements. Most people receiving Medicaid already work, but such requirements in Arkansas and Georgia showed that people often lose coverage under these rules because they have trouble documenting their work hours, including because of technological problems. The nonpartisan Congressional Budget Office estimated an earlier version of the bill would reduce the number of people with Medicaid by at least 8.6 million over a decade. The requirements also could add a burden for employers. The bill’s work requirements are relatively broad and would affect people who are 19 to 64 years old.
- People whose Medicaid coverage is canceled also would no longer qualify for ACA subsidies for marketplace plans. Medicare also would be affected, because the bill would be expected to trigger an across-the-board sequestration cut.
- The bill also would impact abortion by effectively banning it in ACA marketplace plans, which would disrupt a compromise struck in the 2010 law. And the bill would block funding for Planned Parenthood in Medicaid, although that federal money is used for other care such as cancer screenings, not abortions. In the past, the Senate parliamentarian has said that kind of provision is not allowed under budget rules, but some Republicans want to take the unusual step of overruling the parliamentarian.
- This week, FDA leaders released covid-19 vaccine recommendations in a medical journal. They plan to limit future access to the vaccines to people 65 and older and others who are at high risk of serious illness if infected, and they want to require manufacturers to do further clinical trials to show whether the vaccines benefit healthy younger people. There are questions about whether this is legal, which products would be affected, when this would take effect, and whether it’s ethical to require these studies.
- HHS released a report on chronic disease starting in childhood. The report doesn’t include many new findings but is noteworthy in part because of what it doesn’t discuss — gun violence, the leading cause of death for children and teens in the United States; tobacco; the lack of health insurance coverage; and socioeconomic factors that affect access to healthy food.
Also this week, Rovner interviews University of California-Davis School of Law professor and abortion historian Mary Ziegler about her new book on the past and future of the “personhood” movement aimed at granting legal rights to fetuses and embryos.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week they think you should read, too:
Julie Rovner: The Washington Post’s “White House Officials Wanted To Put Federal Workers ‘in Trauma.’ It’s Working,” by William Wan and Hannah Natanson.
Alice Miranda Ollstein: NPR’s “Diseases Are Spreading. The CDC Isn’t Warning the Public Like It Was Months Ago,” by Chiara Eisner.
Anna Edney: Bloomberg News’ “The Potential Cancer, Health Risks Lurking in One Popular OTC Drug,” by Anna Edney.
Sarah Karlin-Smith: The Farmingdale Observer’s “Scientists Have Been Studying Remote Work for Four Years and Have Reached a Very Clear Conclusion: ‘Working From Home Makes Us Happier,’” by Bob Rubila.
Also mentioned in this week’s podcast:
- The New York Times’ “As Congress Debates Cutting Medicaid, a Major Study Shows It Saves Lives,” by Sarah Kliff and Margot Sanger-Katz.
- NBC News’ “Georgia Mother Says She Is Being Forced To Keep Brain-Dead Pregnant Daughter Alive Under Abortion Ban Law,” by Minyvonne Burke.
- The Washington Post’s “Trump and GOP’s Tax Bill Would Force Cuts to Medicare, CBO Says,” by Jacob Bogage and Abha Bhattarai.
- The New England Journal of Medicine’s “An Evidence-Based Approach to Covid-19 Vaccination,” by Vinay Prasad and Martin A. Makary.
click to open the transcript
Transcript: Bill With Billions in Health Program Cuts Passes House
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello, and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Friday, May 23, at 10 a.m. As always, and particularly this week, news happens fast and things might have changed by the time you hear this. So, here we go.
Today we are joined via videoconference by Alice Miranda Ollstein of Politico.
Alice Miranda Ollstein: Hello.
Rovner: Anna Edney of Bloomberg News.
Anna Edney: Hi, everybody.
Rovner: And Sarah Karlin-Smith of the Pink Sheet.
Sarah Karlin-Smith: Hello there.
Rovner: Later in this episode we’ll have my interview with law professor and abortion historian Mary Ziegler, who has a new book out on the history and possible future of the “personhood” movement. But first, this week’s news.
So, against all odds and many predictions, including my own, the House around 7 a.m. Thursday morning, after being in session all night, passed President [Donald] Trump’s One Big Beautiful Bill — that is its actual, official name — by a vote of 215-214, with one Republican voting present. Before we get into the details of the House-passed bill, what are the prospects for this budget reconciliation bill in this form in the Senate? Very different, I would think.
Ollstein: Yeah, this is not going to come out the way it went in. Senate is already openly talking about a “‘One, Big Beautiful’ Rewrite” — that was the headline at Politico.
And you’re going to see some of the same dynamics. You’re going to see hard-liners saying this doesn’t go far enough, this actually adds a lot to the deficit even with all of the deep cuts to government programs. And you’re going to have moderates who have a lot of people in their state who depend on Medicaid and other programs that are set to be cut who say this goes too far. And so you’re going to have that same push and pull. And the House, barely, by one vote, got this through. And so we’ll see if the Senate is able to do the same.
Rovner: Yeah, so all eyes on [Sen.] John McCain in 2017. This year it could be all eyes on Josh Hawley, I suspect, the very conservative senator from Missouri who keeps saying “Don’t touch Medicaid.”
But back to the House bill. We don’t have official scores yet from the Congressional Budget Office, and we won’t for a while, I suspect. But given some last-minute changes made to pacify conservatives who, as Alice pointed out, said this bill didn’t cut deeply enough, I think it’s clear that if it became law in this form, it would represent the biggest cuts to federal health programs in the 60-year history of Medicare and Medicaid.
Those last-minute changes also took pretty square aim at the Affordable Care Act, too, so much that I think it’s safe to call this even more than a partial repeal of the health law. And Medicare does not go unscathed in this measure, either, despite repeated promises by President Trump on the campaign trail and since he took office.
Let’s take these one at a time, starting with Medicaid. I would note that at a meeting with House Republicans on Tuesday, President Trump told them not to expletive around with Medicaid. You can go look up the exact quote yourself if you like. But apparently he’s OK with the $700 billion plus that would be cut in the bill, which Republicans say is just waste, fraud, and abuse. Where does that money come from? And would Medicaid really continue to cover everyone who’s eligible now, which is kind of what the president and moderate Republicans are promising?
Edney: Well, it sounds like the bulk of it is coming from the work requirements that Alice mentioned earlier. And would it be able to cover them? Sure, but will it? No, in the sense that, as Alice has talked about often on this podcast, it’s basically a time tax. It’s not easy to comply with. All federal regulations, they’re not going to a website and putting in what you did for work. Particularly, if you are a freelancer or something, it can be really difficult to meet all the requirements that they’re looking for. And also, for some people, they just don’t have the ability, even the internet, to be able to do that reliably. So they’re going to save money because people are going to lose their health care.
Rovner: I saw a lot of people referring to them this week not as work requirements anymore but as work reporting requirements. Somebody suggested it was like the equivalent of having to file your income taxes every month. It’s not just check a box and say, I worked this month. It’s producing documentation. And a lot of people have jobs that are inconsistent. They may work some hours some week and other hours the other week. And even people who work for small businesses, that would put an enormous burden on the employers to come up with all this.
Obviously, the CBO thinks that a lot of people won’t be able to do this and therefore people are going to lose their health insurance. But Alice, as you have told us numerous times when we did this in Arkansas, it’s not that people aren’t working — it’s that people aren’t successfully reporting their work.
Ollstein: Right. And we’ve seen this in Georgia, too, where this has been implemented, where there are many different ways that people who are working lose their insurance with this. People who don’t have good internet access struggle. People who have fluctuating work schedules, whether it’s agricultural work, tourism work, things that are more seasonal, they can’t comply with this strict monthly requirement.
So there are numerous reports from the ground of people who should be eligible losing their coverage. And I’ll note that one of the last-minute changes the House made was moving up the start date of the requirements. And I’m hearing a lot of state officials and advocates warn that that gives states less time to set up a system where people won’t fall through the cracks. And so the predicted larger savings is in part because they imagine more people will be kicked off the program.
Rovner: It’s also the most stringent work requirement we’ve seen. It would cover people from age 19 through age 64, like right up until you’re eligible for Medicare. And if you lose Medicaid because you fail to meet these reporting requirements, you’re no longer eligible for a subsidy to buy insurance in the ACA exchange. Is there a policy point to this? Or are they just trying to get the most people off the program so they can get the most savings?
Edney: If you ask Republicans, they would tell you: We’re going to get people back working. We’re going to give them the pride of working — as if people don’t want that on their own. But the actual outcome is not that people end up working more. And there are cases even where they lose their health insurance and can’t work a job they already had. On the surface, and this is why it’s such a popular program, because it seems like it would get more people working. Even a large swath of Democrats support the idea when they just hear the name — of voters. But the actual outcome, that doesn’t happen. People aren’t in Medicaid because they aren’t working.
Rovner: Right. And I get to say for the millionth time, nobody is sitting on their couch living on their Medicaid coverage.
Edney: Right, right.
Rovner: There’s no money that comes with Medicaid. It’s just health insurance. The health providers get paid for Medicaid and occasionally the managed-care companies. But there’s no check to the beneficiary, so there’s no way to live on your Medicaid.
As Alice points out, most of the people who are working and have Medicaid are working at jobs, obviously, that don’t offer employer health insurance. So having, in many cases, as you say, Anna, having Medicaid is what enables you to work.
All right, well, our podcast pals Margot Sanger-Katz and Sarah Kliff have an excellent Medicaid story out this week on a new study that looks very broadly at Medicaid and finds that it actually does improve the health of its beneficiaries. Now this seems logical, but that has been quite a talking point for Republicans for many years, that we spend all this money and it doesn’t produce better health, because we’ve had a lot of studies that have been kind of neither here nor there on this.
Do we finally have proof that Democrats need? Because I have heard, over many years — there was a big Oregon study in 2011 that found that it helped people financially and that it helped their mental health, but there was not a lot of physical health benefit that they saw. Of course, it was a brief. It was like two years. And it takes a longer time to figure out the importance of health insurance. But I’m wondering if maybe the Democrats will finally be able to put down that talking point. I didn’t hear it, actually, as much this week as I have in years past: Why are we spending all this money on Medicaid when we don’t know whether it’s producing better health?
Karlin-Smith: One of the interesting things I thought about this study and sort of the timing of it, post-Obamacare expansion of Medicaid and more younger people being covered, is that it seems to really show that, not only does this study show it saves lives, but it’s really helping these younger populations.
And I think there are some theories as to why it might have been harder to show the economic cost-effectiveness benefits people were looking for before, when you had Medicaid covering populations that were already either severely ill or older. Which doesn’t mean it’s not valuable, right? To provide health coverage to somebody who’s 75 or 80, but unfortunately we have not found the everlasting secret to life yet.
So, but I think for economists who want to be able to show this sort of, as they show in this paper, this “quality-adjusted life year” benefit, this provides some really good evidence of what that expansion of Medicaid — which is a lot of what’s being rolled back, potentially, under the reconciliation process — did, which is, helps younger people be healthier and thus, right, hopefully, ideally, live a higher quality of life, and where you need less health coverage over time, and cost the government less.
It’s quite interesting, for people who want to go look at the graph The New York Times put in their story, of just where Medicaid fits, in terms of other sort of interventions we spend a lot of money on to help save lives. Because I was kind of surprised, given how much health insurance does cover, that it comes out on sort of the lower end, as being a pretty good bargain.
Rovner: Yeah. Well, we don’t have time to get into everything that’s in this bill, and there is a lot. It also includes a full ban of Medicaid coverage for gender-affirming care for both minors and adults. And it cuts reimbursement to states that use their own funds to provide coverage to undocumented people. Is this a twofer for Republicans, saving money while fighting the culture wars?
Edney: Certainly. And I was surprised to see some very liberal states on the immigration front saying: We just have to deal with this. And this really sucks, but we have to balance our budget. And if we’re not going to get those tax dollars, then we aren’t going to be able to offer health insurance to people who are undocumented, or Medicaid to people who are undocumented.
Rovner: Yeah, California, most notably.
Edney: Yeah, California for sure. And they found a way to do it, hit them in the pocketbook, and that that’s a way for them to win the culture war, for sure.
Rovner: Alice, you’ve spent a lot of time looking at gender-affirming care. Were you surprised to see it banned for adults, too? Obviously the gender-affirming care for minors has been a continuing issue for a while.
Ollstein: Yeah, I would say not surprised, because this is sort of a common pattern that we see across different things, including in the abortion space, where first policies are targeted just at minors. That often is more politically palatable. And then it gets expanded to the general population. And so I think, given the wave of state bans on care for minors that we’ve seen, I think a lot of people had been projecting that this was the trajectory.
I think that there’s been some really good reporting from The 19th and other outlets about what an impact this would have. Trans people are disproportionately low-income and dependent on Medicaid, and so this would have really sweeping impacts on a lot of people.
Rovner: Well, turning to the Affordable Care Act, if you thought Republicans weren’t going to try to repeal the health law this time around, you thought wrong. There are a bucket of provisions in this bill that will make the Affordable Care Act coverage both more expensive and harder to get, so much that some analysts think it could reduce enrollment by as much as half of the 24 million people who have it now. Hasn’t someone told Republicans that many of these people are their voters?
Edney: Yeah, that’s a good question. I don’t know what the Republican strategists are telling them. But certainly they needed to save money. And so they found their loopholes and their different things that they thought they could scrape from. And maybe no one will notice? But I don’t think that’s going to happen.
A lot of people suddenly have much higher ACA premiums because of the way they’re going to take away this ability that the insurers have had to silver-load, essentially, the way that they deal with the premium tax credits by setting some of the savings, kind of the cost sharing that they need to do, right into the silver plan, because the silver plan is where the premiums are set off of. And so they were able to offer the plans with lower premiums, essentially, but still get paid for cost-sharing reductions. So they were able to still get that money taken away from them.
Rovner: So let me see if I can do it. It was, and this was something that Trump tried to do in 2017, that he thought was going to hurt the marketplace plans. And it ended up doing the opposite—
Edney: Right.
Rovner: —because it basically shifted money from the insurance companies and the beneficiaries back to the federal government, because it made the premium subsidies bigger.
So I think the point I want to make is that we’ve been talking all year about these extra subsidies that are going to expire, and that will make premiums go up, and the Republicans did not move to extend those subsidies. But this going back to the government paying these cost-sharing reduction payments is going to basically reverse the accidental lowering of premiums that Trump did in 2017. And therefore, raise them again.
So now we have a double whammy. We have premiums going up because the extra subsidies expire, and then we’ll have premiums going up even more because they’re going back to this original cost-sharing reduction. And yet, as we have said many times, a lot of these additional people who are now on the Affordable Care Act are people in the very red states that didn’t expand Medicaid. These are Republican voters.
Karlin-Smith: We haven’t talked a lot about the process of how they got this bill through this week. It was incredibly fast and done literally in the dead of night.
Ollstein: Multiple nights.
Karlin-Smith: So you have to wonder, particularly, if you think back to the last time Republicans tried to overturn Obamacare — and they did come pretty close — eventually, I think, that unpalatableness of taking away health care from so many of their own constituents came back to really hurt them. And you do have to wonder if the jamming was in part to make more people unaware of what was happening. You’d still think there’d be political repercussions later down the line when they realize it. But I think, especially, again, just thinking back on all the years when Republicans were saying Democrats were pushing the ACA through too fast and nobody could read the bill, or their CBO scores. This was a much, much faster version of that, with a lot less debate and public transparency and so forth.
Rovner: Yeah, they went to the Rules Committee at 1 a.m. Wednesday, so Tuesday night. The Rules Committee went until almost 9 o’clock the next evening, just consecutively. And shout out to Rules Committee chairman Virginia Foxx, who sat there for, I think, the entire time. And then they went straight from rules to the floor.
So it’s now Wednesday night at 10 o’clock at night, and then went all the way through and voted, I think, just before 7 a.m. I’ve done a lot of all-nighters in the Capitol. I haven’t seen one that was two nights in a row like this. And I have great admiration for the people who really were up for 48 hours to push this thing through.
Well, finally, let’s remember President Trump’s vow not to touch Medicare. Well, Medicare gets touched in this bill, too. In addition to restricting eligibility for some legal immigrants who are able to get coverage now, and making it harder for some low-income Medicare beneficiaries to get extra financial help, mostly through Medicaid, the bill as a whole is also likely to trigger a 4% Medicare sequester. Because, even all those other health cuts and food stamp cuts and other cuts don’t pay for all the huge tax breaks in the bill. Alice, you pointed that out. Is there any suggestion that this part might give people some pause, maybe when it gets to the Senate?
Edney: I’ve heard the Senate mostly seem upset about Medicaid. And I also feel like this idea that sequestration is coming back up into our consciousness is a little bit new. Like you said, it was pushed through and it was like, Oh, wait, this is enough to trigger sequestration. I think it certainly could become a talking point, because Trump said he would not cut Medicare. I don’t think, if senators are worried about Medicaid — and I think maybe some of us were a little surprised that that is coming from some red-state senators. Medicare is a whole different thing, and in the sense of being even more wildly popular with a lot of members of Congress.
Rovner: Yeah, I think this whole thing hasn’t, you’re right, sort of seeped into the general consciousness yet. Alice, did you want to say something?
Ollstein: Yeah, so a couple things, a couple patterns we’ve seen. So one, there are a lot of lawmakers on the right who have been discrediting the CBO, even in advance of estimates coming out, basically disparaging their methodology and trying to convince the public that it’s not accurate. And so I think that’s both around the deficit projections as well as how many people would be uninsured under different policies. So that’s been one reaction to this.
We’ve seen a pattern over many administrations where certain politicians are very concerned about things adding to the deficit when the opposition party is in power. And suddenly those concerns evaporate when their own party is in power and they don’t mind running up the deficit if it’s to advance policies that they want to advance. And so I think, yes, this could bother some fiscal hawks, and we saw that in the House, but I think, also, these other factors are at play.
Rovner: Yeah, I think this has a long way to go. There’s still a lot that people, I think you’re right, have not quite realized is in there. And we will get to more of it in coming weeks, because this has a long process in the Senate.
All right, well, segueing to abortion, the One Big Beautiful Bill also includes a couple of pretty significant abortion provisions. One would effectively ban abortion and marketplace plans for people with lower incomes. Affordable Care Act plans are not currently a big source of insurance coverage for abortion. Many states already ban abortion from coverage in these plans. But this would disrupt one of the big compromises that ultimately got the ACA passed in 2010.
The other provision would evict Planned Parenthood from the Medicaid program, even though federal Medicaid funds don’t and never have been used for abortions. Many, many Medicaid patients use Planned Parenthood for routine medical care, including contraception and cancer screenings, and that is covered by Medicaid.
But while I see lots of anti-abortion groups taking victory laps over this, when the House passed a similar provision in 2017 as part of its repeal bill, the Senate parliamentarian ruled that it could not go in a budget reconciliation bill, because its purpose was not, quote, “primarily budgetary.” So is this all for show? Or is there a belief that something different might happen this time?
Ollstein: Well, I think there is more interest in ignoring or overruling the parliamentarian among Senate Republicans than there has been in the past. We’re seeing that now on an unrelated environmental issue. And so that could signal that they’re willing to do it more in the future. Of course, things like that cut both ways, and that raises the idea that the Democrats could also do that the next time they’re in power.
Rovner: And we should say, that if you overrule the parliamentarian in reconciliation — it’s a she right now — when she says it can’t go in reconciliation, that is equivalent to getting rid of the filibuster.
Ollstein: Correct.
Rovner: So I mean, that’s why both parties say, We want to keep the filibuster. But the moment you say, Hey, parliamentarian, we disagree with you and we’re just going to ignore that, that has ramifications way beyond budget reconciliation legislation.
Ollstein: That’s right. And so that’s been a line that a lot of senators have not been willing to cross, but I think you’re seeing more willingness than before. So that’s definitely something to watch on that. But I think, in terms of abortion, I think this is a real expansion of trends that were already underway, in ever-expanding the concept of what federal dollars going to abortion means. And it’s now in this very indirect way, where it’s reaching into the private insurance market, and it’s using federal funding as a cudgel to prevent groups like Planned Parenthood, and then also these private plans, from using other non-federal money to support abortions. And so it’s a real expansion beyond just you can’t use federal money to pay directly for abortions.
Rovner: Well, meanwhile, two other reproductive-associated health stories worth mentioning. In California, a fertility clinic got bombed. The bomber apparently died in the explosion, but this is the first time I can remember a purposeful bombing to a health center that was not an abortion clinic. How significant is it to the debate, that we’re now seeing fertility clinics bombed as well? And what do we know, if anything, about why the bomber went after a fertility clinic?
Karlin-Smith: There has been, obviously, some pressure on the right, I think, to go after fertility processes, and IVF [in vitro fertilization], and lump that in with abortion. Although, I think Trump and others have pushed back a bit on that, realizing how common and popular some of these fertility treatments are. And also it conflicts, I think, to some extent with their desire to grow the American population.
The motives of this particular person don’t seem aligned with, I guess, the anti-abortion movement. He sort of seems more anti-natalist movement and stuff. So from that perspective, I didn’t see it as being aligned with kind of a bigger, more common political debate we’ve had recently, which is, again, does the Republican Party want to expand the anti-abortion debate even further into fertility treatments and stuff.
Rovner: I was going to say, it certainly has drawn fertility clinics into the abortion debate, even if neither side in the abortion debate would presumably have an interest in blowing up a fertility clinic. But it is now sort of, I guess, in the general consciousness of antisocial people, if you will, that’s out there.
The other story in the news this week is about a woman named Adriana Smith, a nurse and mother from Georgia who was nine weeks pregnant in February when she was declared brain-dead after a medical emergency. Smith has been kept alive on life support ever since, not because her family wants that but because her medical team at Emory University Hospital is worried about running afoul of Georgia’s abortion ban, which prohibits terminations after cardiac activity can be detected. Even if the mother is clinically dead? I feel like this case could have really ominous repercussions at some point.
Ollstein: Well, I just want to point out that, yes, the state’s abortion ban is playing a role here, but this was happening while Roe v. Wade was still in place. There were cases like this. Some of it has to do with legislation around advanced directives and pregnancy. So I will point out that this is not solely a post-Dobbs phenomenon.
Rovner: Yeah, I think it also bears watching. Well, there was lots of vaccine news this week — I’m so glad we have Anna and Sarah here — with both the HHS [Department of Health and Human Services] and FDA [Food and Drug Administration] declaring an end to recommending covid vaccines for what seems to be most of the population. Sarah, what did they do? And what does this mean?
Karlin-Smith: So the new director of FDA’s biologics center and the FDA commissioner released a framework for approving covid shots moving forward. And basically they are saying that, because covid, the virus, shifts, and we want to try and update our vaccines at least yearly, usually, to keep up with the changing viruses, but we want to do that in a reasonable time so that by the time when you update the vaccine it’s actually available within that time — right? — FDA has allowed companies to do studies that don’t require full clinical trials anymore, because we sort of have already done those trials. We know these vaccines are safe and effective. We’re making minor tweaks to them, and they do immunogenicity studies, which are studies that basically show they mount the proper immune response. And then they approve them.
FDA is now, seems to be, saying, We’re only going to allow those studies to approve new covid vaccine updates for people who are over 65, or under 65 and have health conditions, because they are saying, in their mind, the risk-benefit balance of offering these shots doesn’t necessarily pan out favorably for younger, healthier populations, and we should do clinical trials.
It’s not entirely clear yet, despite them rolling out a framework, how this will actually play out. Can they relabel shots already approved? Will this only impact once companies do need to do a strain change next as the virus adapts? Did they go about doing this in a sort of legal manner? It came out through a journal kind of editorial commentary piece, not through the Federal Register or formal guidance. There’s been no notice of comment.
So there’s a lot of questions to remain as to how this will be implemented, which products it would affect, and when. But there is a lot of concern that there may be reduced access to the products moving forward.
Rovner: That’s because the vaccine makers aren’t going to — it’s not probably worth it financially to them — to remount all these studies. Right?
Karlin-Smith: First off, a lot of people I’ve talked to, and this came up yesterday at a meeting FDA had, don’t believe it’s actually ethical to do some of the studies FDA is now calling for. Even though the benefits, particularly when you’re talking about boosting people who already had a primary vaccination series for covid, or some covid, is not the same as the benefits of getting an original covid vaccine series.
There still are benefits, and there still are benefits for pretty much everybody that outweigh the risks. On average, these are extremely safe shots. We know a lot about their safety, and the balance is positive. So people are saying, once that exists, you cannot ethically test it on placebo. Even as [FDA Commissioner Marty] Makary says, Well, so many Americans are declining to take the shot, so let’s test it and see. A lot of ethicists would say it’s actually, even if people are willing to do something that may not be ideal for their health, that doesn’t mean it’s ethical to test it in a trial.
So, I think there’s questions about, just, ethics, but also, right, whether companies would want to invest the time and money it would take to achieve and try to do them under this situation. So that is a big elephant in the room here. And I think some people feel like this is just sort of a push by Makary and his new CBER [Center for Biologics Evaluation and Research] director, essentially, to cut off vaccine access in a little bit of a sneaky way.
Rovner: Well, I did see, also this week, was I think it was Moderna, that was going to make a combination flu covid vaccine, has decided not to. I assume that’s related to all of this?
Karlin-Smith: Right. So Moderna had a, what people call a next-generation vaccine, which is supposed to be an improved update over the original shot, which is a bigger deal than just making a strain change. They actually think they provide a better response to protecting against the virus. And then they also added flu vaccine into it to sort of make it easier for people to get protected from both, and also provided solid data to show it would work well for flu.
And they seem to have probably pulled their application at this point over, again, these new concerns, and what we know Novavax went through in trying to get their covid vaccine across the finish line dealing with this new administration. So I think people have their sort of alert lights up going forward as to how this administration is going to handle vaccine approvals and what that will mean for access going forward.
Rovner: Well, in somewhat related news, we got the long-awaited report from Health and Human Services Secretary Robert F. Kennedy Jr.’s Make America Healthy Again Commission, which is supposed to lay out a blueprint for an action plan that will come later this summer. Not much in the 68-page report seems all that surprising. Some is fairly noncontroversial, calling for more study of ultra-processed foods and less screen time and more physical activity for kids.
And some is controversial but at this point kind of predictable, calling for another look at the childhood vaccine schedule, including, as we just discussed, more placebo studies for vaccines, and also less fluoride available, except in toothpaste. Anything jump out at you guys from the report that we should keep an eye on?
Karlin-Smith: I think one thing to think about is what it doesn’t address and doesn’t talk about. It’s not surprising the issues they call out for harming health in America, and some of them are debatable as to how much they do or don’t harm health, or whether their solutions would actually address those problems.
But they never talk about the U.S.’ lack of a health insurance system that assures people have coverage. They don’t mention the Republican Party’s and likely president’s willingness to sign onto a major bill that’s going to impact health. They don’t really talk about the socioeconomic drivers that impact health, which I find particularly interesting when they talk about food, because, obviously, the U.S. has a lot of healthy and unhealthy food available. And a lot of people know sort of how they could make better choices, but there are these situational factors outside of, often, an individual’s control to lead to that.
And I think the other thing that jumped out to me is, I think The Washington Post had a good line in their paragraph about just how many of the points are either overstated or misstated scientific findings. And they did a pretty good job of going through some of those. And it’s a difficult situation, I think, for the public to grapple with when you have leadership and the top echelons of our health department that is pushing so much misinformation, often very carefully, and having to weed out what is correct, where is the grains of truth, where does it go off into misinformation.
I don’t know. I find it really hard as a journalist. And so I do worry about, again, how this all plays into public perception and misunderstanding of these topics.
Rovner: And apparently they forgot about gun violence in all of this, which is rather notably not there.
Ollstein: Cars and guns are the big killers. And yeah, no mention of that.
Edney: I thought another glaring omission was tobacco. Kids are using e-cigarettes at high rates. We don’t really know much about them. And to Sarah’s point about misinformation, too, I think the hard part of being able to discern a lot of this, even as a member of the public, is everything they’ve done so far is only rhetoric. There hasn’t been actual regulation, or — this could be anything that you’re talking about. It could be food dyes. It could be “most favored nations.” We don’t know what they actually want to implement and what the potential for doing so — I think maybe on vaccines we’re seeing the most action. But as Sarah mentioned, we don’t know how that, whether it legally is going to be something that they can continue doing.
So even with this report, it was highly anticipated, but I don’t think we got anything beyond what I probably heard Kennedy say over and over throughout the campaign and in his bid for health secretary. So I am wondering when they actually decide to move into the policymaking part of it, instead of just telling us they’re going to do something.
Rovner: And interestingly, Secretary Kennedy was interviewed on CNN last night and walked back some of the timelines, even, including that vow that they were going to know the cause of autism by September and that they were going to have an action plan for this ready in another, I think, a hundred days. So this is going to be a hurry-up-and-wait.
All right, well, that is as much news as we have time for in this incredibly busy week. Now we will play my interview with law professor and abortion historian Mary Ziegler, and then we will come back and do our extra credits.
I am pleased to welcome back to the podcast Mary Ziegler, the Martin Luther King Jr. professor of law at the University of California-Davis. She’s also a historian of the abortion movement. And her newest book, just out, is called “Personhood: The New Civil War Over Reproduction.”
Mary Ziegler, thanks for joining us again.
Mary Ziegler: Thanks for having me.
Rovner: So we’ve talked about personhood a lot on our podcast, including with you, but it means different things to different people. What’s your working definition, at least for the purpose of this book?
Ziegler: Yeah, I’m interested in this book in the legal fight for personhood, right? Some people have religious ideas of personhood. Bioethicists have ideas of personhood. Philosophers debate personhood. But I’m really interested in the legal claim that the word “person” in the 14th Amendment, which gives us liberty and equality, applies the moment an egg is fertilized. Because it’s that legal claim that’s had a lot of knock-on effects with abortion, with IVF, and potentially even beyond.
Rovner: So if we as a society were to accept that fetuses or embryos or zygotes were people with full constitutional rights at the moment of creation, that can impact things way beyond abortion, right?
Ziegler: Definitely, yeah, especially if you make the moves that the anti-abortion movement, or the pro-life movement, in the United States has made, right? So one of the other things that’s probably worth saying is, if you believe the claim I laid out about fetal personhood, that doesn’t mean you necessarily think abortion should be criminalized or that IVF should be criminalized, either.
But the people who are leading the anti-abortion movement do, in large part, right? So it would have ramifications in lots of other contexts, because there’s a conclusion not only that human life begins at fertilization and that constitutional rights begin at fertilization but that the way you honor those constitutional rights is primarily by restricting or criminalizing certain things that threaten that life, in the views of the people who advocate for it.
Rovner: Right. And that includes IVF and forms of contraception. That’s where we sort of get to this idea that an abortion is murder or that, in this case, doing anything that harms even a zygote is murder.
Ziegler: Yeah. And it gets us to the Adriana Smith case in Georgia, too. So there’s sort of end-of-life cases that emerge. So, it obviously would have a big impact on abortion. So it’s not wrong to think about abortion in this context. It’s just that would definitely not be the stopping point.
Rovner: So, many people have only talked about personhood, really, since the Supreme Court overturned Roe in 2022, but the concept is a lot older than that. I started covering personhood in like 2010, I think, when a couple of states were trying to vote on it. I didn’t realize until I read your book that it goes back well beyond even that.
Ziegler: Yeah. So I think a lot of people had that conception. And in the 2010s, there were state constitutional amendment efforts to write the idea of fetal personhood into state constitutions. And they all failed. So I think the narrative coming out of that was that you had the anti-abortion movement on the one hand, and then you had this more extreme fetal personhood movement on the other hand.
And that narrative fundamentally is wrong. There is no one in the anti-abortion movement who’s opposed to fetal personhood. There are disagreements about how and when it can be recognized. There’s strategic disagreements. There are no substantive disagreements much to speak of on the basics of fetal personhood.
So the idea goes all the way back to the 1960s, when states were first reforming the 19th-century criminal laws you sometimes see coming back to life as zombie laws. And initially it started as a strategic necessity, because it was very hard for the early anti-abortion movement to stop this reform wave, right? They were saying things like, Oh, abortion is going to lead to more sexual promiscuity, or, No one really needs abortion, because pregnancy is no longer dangerous. And that just wasn’t getting the job done.
So they began to argue that no one had a choice to legalize abortion in worse circumstances, because it would violate the rights of the unborn child. What’s interesting is that argument went from being this kind of strategic expedient to being this tremendously emotionally resonant long-term thing that has lived on the American right for now like a half-century. Even in moments when, I think arguably like right now, when it’s not politically smart to be making the argument, people will continue to, because this speaks to something, I think, for a lot of people who are opposed to abortion and other things like IVF.
Rovner: I know you’ve got access in writing this book to a lot of internal documents from people in the anti-abortion movement. I’m jealous, I have to say. Was there something there that surprised you?
Ziegler: Yeah, I think I was somewhat surprised by how much people talked this language of personhood when they were alone, right? This was not just something for the consumption of judges, or the consumption of politicians, or sort of like a nicer way to talk about what people really wanted. This was what people said when there was no one else there.
That didn’t mean they didn’t say other things that suggested that there were lots of other values and beliefs underlying this concept of personhood. But I think one of the important lessons of that is if you’re trying to understand people who are opposed to abortion, just assuming that everything they’re saying is just pure strategy is not helpful, right? Any more than it would be for people who support reproductive rights, to have it assume that everything they’re saying is not genuine. You just fail to understand what people are doing, I think. And I think that was probably what I was the most surprised about.
Rovner: I was struck that you point out that personhood doesn’t have to begin and end with the criminalization of abortion. How could more acceptance of the rights of the unborn change society in perhaps less polarized ways?
Ziegler: Yeah, one of the things that’s really striking is that there are other countries that recognize a right to life for a fetus or unborn child that don’t criminalize abortion or don’t enforce criminal abortion laws. And often what they say is that it’s not OK for the state to start with criminalization when it isn’t doing things to support pregnant women, who after all are necessary for a fetus or unborn child to survive, right?
So there are strategies that you could use to reduce infant mortality, for example, to reduce neonatal mortality, to reduce miscarriage and stillbirth, to improve maternal health, to really eliminate some of the reasons that people who may want, all things being equal, to carry a child to term. That’s not, obviously, going to be everybody. Some people don’t want to be parents at all.
But there are other people for whom it’s a matter of resources, or it’s a matter of overcoming racial discrimination, or it’s a matter of leaving an abusive relationship. And if governments were more committed to doing some of those things, it’s reasonable to assume that a subset of those people would carry pregnancies to term, right?
So there are lots of ways that if a state were serious about honoring fetal life, that it could. I think one of the other things that’s striking that I realized in writing the book is that that tracks with what a subset of Americans think. You’ll find these artifacts in polls where you’ll get something like 33% of people in Pew Forum’s 2022 poll saying they thought that life and rights began at conception, but also that abortion shouldn’t be criminalized.
So there are a subset of Americans who, whether they’re coming from a place of faith or otherwise, can hold those two beliefs at once. So I think an interesting question is, could we have a politics that accommodates that kind of belief? And at the moment the answer is probably not, but it’s interesting to imagine how that could change.
Rovner: It’s nice to know that there is a place that we can hope to get.
Ziegler: Yeah, exactly.
Rovner: Mary Ziegler, thank you so much for joining us again.
Ziegler: Thanks for having me.
Rovner: OK, we’re back. And now it’s time for our extra-credit segment. That’s where we each recognize a story we read this week we think you should read, too. Don’t worry if you miss it. We will put the links in our show notes on your phone or other mobile devices. Sarah, you chose first this week. You go first.
Karlin-Smith: I purposely chose a sort of light story from Australia, where scientists studied remote work, and the headline is “[Scientists Have Been Studying Remote Work for Four Years and Have] Reached a Very Clear Conclusion: ‘Working From Home Makes Us Happier.’” And it just goes through some of the benefits and perks people have found from working remotely, including more sleep, more time with friends and family, things like that. And it just felt like a nice, interesting read in a time where there’s a lot of heavy health news.
Rovner: Also, scientific evidence of things that I think we all could have predicted. Anna.
Edney: Apologies for going the other direction here, but it’s a story that I wrote this week, an investigation that I’ve been working on for a long time, “The Potential Cancer, Health Risks Lurking in One Popular OTC Drug.” So this is one, in particularly a lot of women have used. You can go in any CVS, Target, Walmart, stores like that, and buy it. Called Azo, for urinary tract infections. And all these stores sell their own generic versions as well, under phenazopyridine.
And this drug, I was kind of shocked to learn, is not FDA-approved. There are prescription versions that are not FDA-approved, either. It’s just been around so long that it’s been grandfathered in. And that may not be a big deal, except that this one, the FDA has raised questions about whether it causes cancer and whether it needs a stronger cancer warning, because the National Cancer Institute found in 1978 that it causes tumors in rats and mice. But no other work has been done on this drug, because it hasn’t been approved. So no one’s looked at it in humans. And it masks issues that really need antibiotics and causes a host of other issues.
There were — University of Virginia toxicologists told me they found, in the last 20 years, at least 200 suspected teen suicides where they used this drug, because of how dangerous this drug can be in any higher amounts than what’s on the box. So I went through this drug, but there are other ones on the market as well that are not approved. And there’s this whole FDA system that has allowed the OTC [over-the-counter] market to be pretty lax.
Rovner: OK, that’s terrifying. But thank you for your work. Alice.
Ollstein: Speaking of terrifying, I chose a piece from NPR called, “Diseases Are Spreading. The CDC Isn’t Warning the Public Like It Was Months Ago.” And this is a look at all of the ways our public health agency that is supposed to be letting us know when outbreaks are happening, and where, and how to protect ourselves, they’ve gone dark. They are not posting on social media. They are not sending out alerts. They are not sending out newsletters. And it walks through the danger of all of that happening, with interviews with people who are still on the inside and on the outside experiencing the repercussions.
Rovner: Well, my extra credit, it helps explain why Alice’s extra credit, because it’s about all the people who were doing that who have been fired or laid off from the federal government. It’s called, “White House Officials Wanted To Put Federal Workers ‘in Trauma.’ It’s Working,” by William Wan and Hannah Natanson.
And it’s the result of interviews with more than 30 current and former federal workers, along with the families of some who died or killed themselves. And it’s a review of documents to confirm those stories. It’s a super-depressing but beautifully told piece about the dramatic mental health impact of the federal DOGE [Department of Government Efficiency] layoffs and firings, and the impact that that’s been having on these workers, their families, and their communities.
OK, that is this week’s show. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review. That helps other people find us, too. Thanks to our fill-in editor this week, Rebecca Adams, and our producer, Francis Ying. Also, as always, you can email us your comments or questions. We’re at whatthehealth@kff.org. Or you can find me on X, @jrovner, or on Bluesky, @julierovner. Where are you guys hanging these days? Anna?
Edney: Both of those [X and Bluesky], @annaedney.
Rovner: Sarah.
Karlin-Smith: Everywhere — X, Bluesky, LinkedIn, @SarahKarlin or @sarahkarlin-smith.
Rovner: Alice.
Ollstein: @AliceOllstein on X and @alicemiranda on Bluesky.
Rovner: I am off to California next week, where we’ll be taping the podcast at the annual meeting of the Association for Health Care Journalists, which we won’t post until the following Monday. So everyone please have a great Memorial Day holiday week. And until then, be healthy.
Credits
Francis Ying
Audio producer
Rebecca Adams
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
2 months 1 day ago
california, COVID-19, Health Care Costs, Insurance, Medicaid, Medicare, Multimedia, Public Health, States, The Health Law, Abortion, Children's Health, FDA, HHS, KFF Health News' 'What The Health?', Medicaid Expansion, Misinformation, Nutrition, Podcasts, Pregnancy, Premiums, reproductive health, Subsidies, Transgender Health, U.S. Congress, vaccines, Women's Health

Republicanos buscan castigar a estados que ofrecen seguro de salud a inmigrantes sin papeles
La emblemática legislación del presupuesto del presidente Donald Trump castigaría a 14 estados que ofrecen cobertura de salud a personas que viven en el país sin papeles.
Estos estados, la mayoría liderados por demócratas, dan seguro médico a algunos inmigrantes de bajos ingresos —a menudo niños—, independientemente de su estatus migratorio. Defensores argumentan que la política es humanitaria y que, en última instancia, ahorra costos.
Sin embargo, la legislación federal, que los republicanos han denominado One Big Beautiful Bill (Un hermoso gran proyecto de ley), recortaría drásticamente los reembolsos federales de Medicaid a esos estados en miles de millones de dólares anuales en total, a menos que reduzcan esos beneficios.
El proyecto de ley fue aprobado por un estrecho margen en la Cámara de Representantes el jueves 22 de mayo, y ahora pasa al Senado.
Si bien avanza gran parte de la agenda nacional de Trump, incluyendo grandes recortes de impuestos que benefician principalmente a los estadounidenses más ricos, la legislación también realiza recortes sustanciales del gasto en Medicaid que, según los responsables del presupuesto del Congreso, dejará a millones de personas de bajos ingresos sin seguro médico.
De ser aprobados por el Senado, estos recortes representarían un complejo obstáculo político y económico para los estados y Washington, DC, que utilizan sus propios fondos para brindar seguro médico a algunas personas que viven en Estados Unidos sin autorización.
Estos estados verían reducidos en 10 puntos porcentuales los reembolsos federales para las personas cubiertas por la expansión de Medicaid que se realize bajo la Ley de Cuidado de Salud a Bajo Precio (ACA).
Estos recortes le costarían a California, el estado que más tiene que perder, hasta $3 mil millones al año, según un análisis de KFF, una organización sin fines de lucro dedicada a información de salud que incluye a KFF Health News.
En conjunto, los 15 lugares afectados (los 14 estados y DC) cubren a aproximadamente 1.9 millones de inmigrantes sin papeles, según KFF. La entidad indica que la sanción también podría aplicarse a otros estados que cubren a inmigrantes con residencia legal.
Dos de los estados, Illinois y Utah, tienen leyes de “activación” que exigen terminar con sus expansiones de Medicaid si el gobierno federal reduce su aporte de fondos. Esto significa que, a menos que esos estados deroguen sus leyes de activación o dejen de cubrir a las personas sin estatus migratorio legal, muchos más estadounidenses de bajos ingresos podrían quedarse sin seguro.
Si continúan cubriendo a personas sin papeles, a partir del año fiscal 2027, los estados restantes y Washington, DC, tendrían que aportar millones o miles de millones de dólares adicionales cada año, para compensar las reducciones en sus reembolsos federales de Medicaid.
Después de California, Nueva York podría perder la mayor parte de la financiación federal: cerca de 1.600 millones de dólares anuales, según KFF.
El senador estatal de California, Scott Wiener, demócrata y presidente del Comité de Presupuesto del Senado, afirmó que la legislación de Trump ha sembrado el caos mientras los legisladores estatales trabajan para aprobar su propio presupuesto antes del 15 de junio.
“Tenemos que mantenernos firmes”, declaró. “California ha decidido que queremos una atención médica universal y que vamos a garantizar que todos tengan acceso a la atención médica, y que no vamos a permitir que millones de personas indocumentadas reciban atención primaria en salas de emergencia”.
El gobernador de California, el demócrata Gavin Newsom, declaró en un comunicado que el proyecto de ley de Trump devastaría la atención médica en su estado.
“Millones de personas perderán cobertura, los hospitales cerrarán y las redes de seguridad social podrían colapsar bajo ese peso”, dijo Newsom.
En su propuesta de presupuesto del 14 de mayo, Newsom instó a los legisladores a recortar algunos beneficios para inmigrantes sin papeles, citando el aumento desmedido de los costos del programa estatal de Medicaid. Si el Congreso recorta los fondos para la expansión de Medicaid, el estado no estaría en condiciones de cubrir los gastos, afirmó el gobernador.
Newsom cuestionó si el Congreso tiene la autoridad para penalizar a los estados por cómo gastan su propio dinero, y afirmó que su estado consideraría impugnar la medida en los tribunales.
El representante estatal de Utah, Jim Dunnigan, republicano que ayudó a impulsar un proyecto de ley para cubrir a los niños en su estado independientemente de su estatus migratorio, afirmó que Utah necesita mantener la expansión de Medicaid que comenzó en 2020.
“No podemos permitirnos, ni monetaria ni políticamente, que se recorten nuestros fondos federales para la expansión”, declaró. Dunnigan no especificó si cree que el estado debería cancelar su cobertura para inmigrantes si la disposición republicana sobre sanciones se convierte en ley.
El programa de Utah cubre a unos 2.000 niños, el máximo permitido por su ley. Los inmigrantes adultos sin estatus legal no son elegibles. La expansión de Medicaid de Utah cubre a unos 75.000 adultos, quienes deben ser ciudadanos o inmigrantes con residencia legal.
Matt Slonaker, director ejecutivo del Utah Health Policy Project, una organización de defensa del consumidor, afirmó que el proyecto de ley de la Cámara federal deja al estado en una posición difícil.
“Políticamente, no hay grandes alternativas”, declaró. “Es el dilema del prisionero: cualquier movimiento en cualquier dirección no tiene mucho sentido”.
Slonaker apuntó que un escenario probable es que los legisladores estatales eliminen su ley de activación, y luego encuentren la manera de compensar la pérdida de fondos federales para la expansión.
Utah ha financiado su parte del costo de la expansión de Medicaid con impuestos sobre las ventas y los hospitales.
“El Congreso pondría al estado de Utah en posición de tener que tomar una decisión política muy difícil”, declaró Slonaker.
En Illinois, la sanción del Partido Republicano tendría incluso consecuencias más graves. Esto se debe a que podría llevar a que 770.000 adultos perdieran la cobertura médica que obtuvieron con la expansión estatal de Medicaid.
Stephanie Altman, directora de justicia sanitaria del Shriver Center on Poverty Law, un grupo de defensa con sede en Chicago, afirmó que es posible que su estado, liderado por demócratas, derogue su ley de activación antes de permitir que se dé por terminada la expansión de Medicaid.
Agregó que el estado también podría eludir la sanción solicitando a los condados que financien la cobertura para inmigrantes. “Obviamente, sería una situación difícil”, declaró.
Altman indicó que el proyecto de ley de la Cámara de Representantes parece redactado para penalizar a los estados controlados por demócratas, ya que estos suelen brindar cobertura a inmigrantes sin importar su estatus migratorio.
Agregó que la disposición demuestra la “hostilidad de los republicanos contra los inmigrantes” y que “no quieren que vengan aquí y reciban cobertura pública”.
Mike Johnson, el presidente de la Cámara de Representantes de Estados Unidos, declaró en mayo que los programas estatales que brindan cobertura pública a personas sin importar su estatus migratorio actúan como un “felpudo abierto”, invitando a más personas a cruzar la frontera sin autorización. Afirmó que los esfuerzos para eliminar estos programas cuentan con el apoyo de las encuestas públicas.
Una encuesta de Reuters-Ipsos realizada entre el 16 y el 18 de mayo reveló que el 47% de los estadounidenses aprueba las políticas migratorias de Trump y el 45% las desaprueba. La encuesta reveló que el índice de aprobación general de Trump ha caído 5 puntos porcentuales desde que regresó al cargo en enero, hasta el 42%, con un 52% de los estadounidenses desaprobando su gestión.
ACA, también conocida como Obamacare, impulsó a los estados a ampliar Medicaid a adultos con ingresos de hasta el 138% del nivel federal de pobreza, o $21.597 por persona este año. Cuarenta estados y Washington, DC, ampliaron su cobertura, lo que contribuyó a reducir la tasa nacional de personas sin seguro a un mínimo histórico.
El gobierno federal ahora cubre el 90% de los costos de las personas incluidas en Medicaid gracias a la ampliación del Obamacare.
En los estados que cubren la atención médica de inmigrantes sin autorización, el proyecto de ley republicano reduciría la contribución del gobierno federal del 90% al 80% del costo de la cobertura para cualquier persona que se incorpore a Medicaid bajo la expansión de ACA.
Por ley, los fondos federales de Medicaid no pueden utilizarse para cubrir a personas que se encuentran en el país papeles, excepto para servicios de embarazo y emergencias.
Los otros estados que utilizan sus propios fondos para cubrir a personas sin importar su estatus migratorio son: Colorado, Connecticut, Maine, Massachusetts, Minnesota, Nueva Jersey, Oregon, Rhode Island, Vermont y Washington, según KFF.
Ryan Long, director de relaciones con el Congreso del Paragon Health Institute, un influyente grupo político conservador, afirmó que incluso si utilizan sus propios fondos para la cobertura de inmigrantes, los estados aún dependen de los fondos federales para “apoyar sistemas que faciliten la inscripción de inmigrantes indocumentados”.
Long afirmó que la preocupación por que los estados con leyes de activación puedan ver finalizada la expansión de Medicaid es una “pista falsa”, ya que los estados tienen la opción de eliminar sus activadores, como hizo Michigan en 2023.
La sanción por ofrecer cobrtura de salud a personas en el país sin papeles es una de las distintas maneras en que el proyecto de ley de la Cámara de Representantes recorta el gasto federal en Medicaid.
La legislación también trasladaría más costos de Medicaid a los estados al exigirles que verifiquen si los adultos cubiertos por el programa trabajan. Los estados también tendrían que recertificar la elegibilidad de los beneficiarios de la expansión de Medicaid cada seis meses, en lugar de una vez al año o menos, como lo hacen actualmente la mayoría.
El proyecto de ley también congelaría la práctica de los estados de gravar con impuestos a hospitales, residencias de adultos mayores, planes de atención médica administrada y otras compañías de atención médica para financiar su parte de los costos de Medicaid.
En una estimación preliminar del 11 de mayo, la Oficina de Presupuesto del Congreso (CBO) indicó que, según el proyecto de ley aprobado por la Cámara de Representantes, alrededor de 8,6 millones de personas más perderían la cobertura médica en 2034.
Esa cifra aumentará a casi 14 millones, según la CBO, después que la administración Trump finalice las nuevas regulaciones de ACA y, si el Congreso, liderado por los republicanos, como se prevé, se niegue a extender los subsidios mejorados para ayudar a pagar las primas de los planes de salud comerciales vendidos a través de los mercados del Obamacare.
Los subsidios mejorados, una prioridad del ex presidente Joe Biden, eliminaron por completo las primas mensuales para algunas personas que adquirieran planes de Obamacare. Y expiran a fin de año.
Esta historia fue producida por Kaiser Health News, que publica California Healthline, un servicio editorialmente independiente de la California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
2 months 1 day ago
Health Care Costs, Insurance, Medi-Cal, Medicaid, Noticias En Español, Race and Health, States, The Health Law, Uninsured, california, District Of Columbia, Latinos, Legislation, Minnesota, New Jersey, New York, Rhode Island, Utah, Washington
Republicans Aim To Punish States That Insure Unauthorized Immigrants
President Donald Trump’s signature budget legislation would punish 14 states that offer health coverage to people in the U.S. without authorization.
The states, most of them Democratic-led, provide insurance to some low-income immigrants — often children — regardless of their legal status. Advocates argue the policy is both humane and ultimately cost-saving.
President Donald Trump’s signature budget legislation would punish 14 states that offer health coverage to people in the U.S. without authorization.
The states, most of them Democratic-led, provide insurance to some low-income immigrants — often children — regardless of their legal status. Advocates argue the policy is both humane and ultimately cost-saving.
But the federal legislation, which Republicans have titled the “One Big Beautiful Bill,” would slash federal Medicaid reimbursements to those states by billions of dollars a year in total unless they roll back the benefits.
The bill narrowly passed the House on Thursday and next moves to the Senate. While enacting much of Trump’s domestic agenda, including big tax cuts largely benefiting wealthier Americans, the legislation also makes substantial spending cuts to Medicaid that congressional budget scorekeepers say will leave millions of low-income people without health insurance.
The cuts, if approved by the Senate, would pose a tricky political and economic hurdle for the states and Washington, D.C., which use their own funds to provide health insurance to some people in the U.S. without authorization.
Those states would see their federal reimbursement for people covered under the Affordable Care Act’s Medicaid expansion cut by 10 percentage points. The cuts would cost California, the state with the most to lose, as much as $3 billion a year, according to an analysis by KFF, a health information nonprofit that includes KFF Health News.
Together, the 15 affected places cover about 1.9 million immigrants without legal status, according to KFF. The penalty might also apply to other states that cover lawfully residing immigrants, KFF says.
Two of the states — Utah and Illinois — have “trigger” laws that call for their Medicaid expansions to terminate if the feds reduce their funding match. That means unless those states either repeal their trigger laws or stop covering people without legal immigration status, many more low-income Americans could be left uninsured.
The remaining states and Washington, D.C., would have to come up with millions or billions more dollars every year, starting in the 2027 fiscal year, to make up for reductions in their federal Medicaid reimbursements, if they keep covering people in the U.S. without authorization.
Behind California, New York stands to lose the most federal funding — about $1.6 billion annually, according to KFF.
California state Sen. Scott Wiener, a Democrat who chairs the Senate budget committee, said Trump’s legislation has sown chaos as state legislators work to pass their own budget by June 15.
“We need to stand our ground,” he said. “California has made a decision that we want universal health care and that we are going to ensure that everyone has access to health care, and that we’re not going to have millions of undocumented people getting their primary care in emergency rooms.”
California Gov. Gavin Newsom, a Democrat, said in a statement that Trump’s bill would devastate health care in his state.
“Millions will lose coverage, hospitals will close, and safety nets could collapse under the weight,” Newsom said.
In his May 14 budget proposal, Newsom called on lawmakers to cut some benefits for immigrants without legal status, citing ballooning costs in the state’s Medicaid program. If Congress cuts Medicaid expansion funding, the state would be in no position to backfill, the governor said.
Newsom questioned whether Congress has the authority to penalize states for how they spend their own money and said his state would consider challenging the move in court.
Utah state Rep. Jim Dunnigan, a Republican who helped spearhead a bill to cover children in his state regardless of their immigration status, said Utah needs to maintain its Medicaid expansion that began in 2020.
“We cannot afford, monetary-wise or policy-wise, to see our federal expansion funding cut,” he said. Dunnigan wouldn’t say whether he thinks the state should end its immigrant coverage if the Republican penalty provision becomes law.
Utah’s program covers about 2,000 children, the maximum allowed under its law. Adult immigrants without legal status are not eligible. Utah’s Medicaid expansion covers about 75,000 adults, who must be citizens or lawfully present immigrants.
Matt Slonaker, executive director of the Utah Health Policy Project, a consumer advocacy organization, said the federal House bill leaves the state in a difficult position.
“There are no great alternatives, politically,” he said. “It’s a prisoner’s dilemma — a move in either direction does not make much sense.”
Slonaker said one likely scenario is that state lawmakers eliminate their trigger law then find a way to make up the loss of federal expansion funding.
Utah has funded its share of the cost of Medicaid expansion with sales and hospital taxes.
“This is a very hard political decision that Congress would put the state of Utah in,” Slonaker said.
In Illinois, the GOP penalty would have even larger consequences. That’s because it could lead to 770,000 adults’ losing the health coverage they gained under the state’s Medicaid expansion.
Stephanie Altman, director of health care justice at the Shriver Center on Poverty Law, a Chicago-based advocacy group, said it’s possible her Democratic-led state would end its trigger law before allowing its Medicaid expansion to terminate. She said the state might also sidestep the penalty by asking counties to fund coverage for immigrants. “It would be a hard situation, obviously,” she said.
Altman said the House bill appeared written to penalize Democratic-controlled states because they more commonly provide immigrants coverage without regard for their legal status.
She said the provision shows Republicans’ “hostility against immigrants” and that “they do not want them coming here and receiving public coverage.”
U.S. House Speaker Mike Johnson said this month that state programs that provide public coverage to people regardless of immigration status serve as “an open doormat,” inviting more people to cross the border without authorization. He said efforts to end such programs have support in public polling.
A Reuters-Ipsos poll conducted May 16-18 found that 47% of Americans approve of Trump’s immigration policies and 45% disapprove. The poll found that Trump’s overall approval rating has sunk 5 percentage points since he returned to office in January, to 42%, with 52% of Americans disapproving of his performance.
The Affordable Care Act, widely known as Obamacare, enabled states to expand Medicaid to adults with incomes of up to 138% of the federal poverty level, or $21,597 for an individual this year. Forty states and Washington, D.C., expanded, helping reduce the national uninsured rate to a historic low.
The federal government now pays 90% of the costs for people added to Medicaid under the Obamacare expansion.
In states that cover health care for immigrants in the U.S. without authorization, the Republican bill would reduce the federal government’s contribution from 90% to 80% of the cost of coverage for anyone added to Medicaid under the ACA expansion.
By law, federal Medicaid funds cannot be used to cover people who are in the country without authorization, except for pregnancy and emergency services.
The other states that use their own money to cover people regardless of immigration status are Colorado, Connecticut, Maine, Massachusetts, Minnesota, New Jersey, Oregon, Rhode Island, Vermont, and Washington, according to KFF.
Ryan Long, director of congressional relations at Paragon Health Institute, an influential conservative policy group, said that even if they use their own money for immigrant coverage, states still depend on federal funds to “support systems that facilitate enrollment of illegal aliens.”
Long said the concern that states with trigger laws could see their Medicaid expansion end is a “red herring” because states have the option to remove their triggers, as Michigan did in 2023.
The penalty for covering people in the country without authorization is one of several ways the House bill cuts federal Medicaid spending.
The legislation would shift more Medicaid costs to states by requiring them to verify whether adults covered by the program are working. States would also have to recertify Medicaid expansion enrollees’ eligibility every six months, rather than once a year or less, as most states currently do.
The bill would also freeze states’ practice of taxing hospitals, nursing homes, managed-care plans, and other health care companies to fund their share of Medicaid costs.
The Congressional Budget Office said in a May 11 preliminary estimate that, under the House-passed bill, about 8.6 million more people would be without health insurance in 2034. That number will rise to nearly 14 million, the CBO estimates, after the Trump administration finishes new ACA regulations and if the Republican-led Congress, as expected, declines to extend enhanced premium subsidies for commercial insurance plans sold through Obamacare marketplaces.
The enhanced subsidies, a priority of former President Joe Biden, eliminated monthly premiums altogether for some people buying Obamacare plans. They are set to expire at the end of the year.
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
2 months 1 day ago
california, Health Care Costs, Insurance, Medicaid, States, Colorado, Connecticut, District Of Columbia, Illinois, Immigrants, Legislation, Maine, Massachusetts, Medicaid Watch, Minnesota, New Jersey, New York, Oregon, Rhode Island, U.S. Congress, Utah, Vermont, Washington
Families of Transgender Youth No Longer View Colorado as a Haven for Gender-Affirming Care
In recent years, states across the Mountain West have passed laws that limit doctors from providing transgender children with certain kinds of gender-affirming care, from prohibitions on surgery to bans on puberty blockers and hormones.
Colorado families say their state was a haven for those health services for a long time, but following executive orders from the Trump administration, even hospitals in Colorado limited the care they offer for trans patients under age 19. KFF Health News Colorado correspondent Rae Ellen Bichell spoke with youth and their families.
GRAND JUNCTION, Colo. — On a Friday after school, 6-year-old Esa Rodrigues had unraveled a ball of yarn, spooked the pet cat, polled family members about their favorite colors, and tattled on a sibling for calling her a “butt-face mole rat.”
Next, she was laser-focused on prying open cherry-crisp-flavored lip gloss with her teeth.
“Yes!” she cried, twisting open the cap. Esa applied the gloopy, shimmery stuff in her bedroom, where a large transgender pride flag hung on the wall.
Esa said the flag makes her feel “important” and “happy.” She’d like to take it down from the wall and wear it as a cape.
Her parents questioned her identity at first, but not anymore. Before, their anxious child dreaded going to school, bawled at the barbershop when she got a boy’s haircut, and curled into a fetal position on the bathroom floor when she learned she would never get a period.
Now, that child is happily bounding up a hill, humming to herself, wondering aloud if fairies live in the little ceramic house she found perched on a stone.
Her mom, Brittni Packard Rodrigues, wants this joy and acceptance to stay. Depending on a combination of Esa’s desire, her doctors’ recommendations, and when puberty sets in, that might require puberty blockers, followed by estrogen, so that Esa can grow into the body that matches her being.
“In the long run, blockers help prevent all of those surgeries and procedures that could potentially become her reality if we don’t get that care,” Packard Rodrigues said.
The medications known as puberty blockers are widely used for conditions that include prostate cancer, endometriosis, infertility, and puberty that sets in too early. Now, the Trump administration is seeking to limit their use specifically for transgender youth.
Esa’s home state of Colorado has long been known as a haven for gender-affirming care, which the state considers legally protected and an essential health insurance benefit. Medical exiles have moved to Colorado for such treatment in the past few years. As early as the 1970s, the town of Trinidad became known as “the sex-change capital of the world” when a cowboy-hat-wearing former Army surgeon, Stanley Biber, made his mark performing gender-affirming surgeries for adults.
On his first day in office, President Donald Trump signed an executive order refuting the existence of transgender people by saying it is a “false claim that males can identify as and thus become women and vice versa.” The following week, he issued another order calling puberty blockers and hormones for anyone under age 19 a form of chemical “mutilation” and “a stain on our Nation’s history.” It directed agencies to take steps to ensure that recipients of federal research or education grants stop providing it.
Subsequently, health care organizations in Colorado; California; Washington, D.C.; and elsewhere announced they would preemptively comply. In Colorado, that included three major health care organizations: Children’s Hospital Colorado, Denver Health, and UCHealth. At the end of January and in early February, the three systems announced changes to the gender-affirming care they provide to patients under 19, effective immediately: no new hormone or puberty blocker prescriptions for patients who hadn’t had them before, limited or no prescription renewals for those who had, and no surgeries, though Children’s Hospital had never offered it, and such surgery is rare among teens: For every 100,000 trans minors, fewer than three undergo surgery.
Children’s Hospital and Denver Health resumed offering puberty blockers and hormones on Feb. 24 and Feb. 19, respectively, after Colorado joined a U.S. District Court lawsuit in Washington state. The court concluded that Trump’s orders relating to gender “discriminate on the basis of transgender status and sex.” It granted a preliminary injunction blocking them from taking effect in the four states involved in the lawsuit.
Surgeries, however, have not resumed. Denver Health said it will “continue its pause on gender-affirming surgeries for patients under 19 due to patient safety and given the uncertainty of the legal and regulatory landscape.”
UCHealth has resumed neither medication nor surgery for those under 19. “Our providers are awaiting a more permanent decision from federal courts that may resolve the uncertainty around providing this care,” spokesperson Kelli Christensen wrote.
Trans youth and their families said the court ruling and the two Colorado health systems’ decisions to resume treatments haven’t resolved matters. It has bought them time to stockpile prescriptions, to try to find private practice physicians with the right training to monitor blood work and adjust prescriptions accordingly, and, for some, to work out the logistics of moving to another state or country.
The Trump administration has continued to press health providers beyond the initial executive orders by threatening to withhold or cancel federal money awarded to them. In early March, the Health Resources and Services Administration said it would review funding for graduate medical education at children’s hospitals.
KFF Health News requested comment from White House deputy press secretary Kush Desai but did not receive a response. HHS deputy press secretary Emily Hilliard responded with links to two prior press releases.
Medical interventions are just one type of gender-affirming care, and the process to get treatment is long and thorough. Researchers have found that, even among those with private insurance, transgender youth aren’t likely to receive puberty blockers and hormones. Interestingly, most gender-affirming breast reduction surgeries performed on men and boys are done on cisgender — not transgender — patients.
Kai, 14, wishes he could have gone on puberty blockers. He lives in Centennial, a Denver suburb. KFF Health News is not using his full name because his family is worried about him being harassed or targeted.
Kai got his period when he was 8 years old. By the time he realized he was transgender, in middle school, it was too late to start puberty blockers.
His doctors prescribed birth control to suppress his periods, so he wouldn’t be reminded each month of his gender dysphoria. Then, once he turned 14, he started taking testosterone.
Kai said if he didn’t have hormone therapy now, he would be a danger to himself.
“Being able to say that I’m happy in my body, and I get to be happy out in public without thinking everyone’s staring at me, looking at me weird, is such a huge difference,” he said.
His mom, Sherry, said she is happy to see Kai relax into the person he is.
Sherry, who asked to use her middle name to prevent her family from being identified, said she started stockpiling testosterone the moment Trump got elected but hadn’t thought about what impact there would be on the availability of birth control. Yet after the executive orders, that prescription, too, became tenuous. Sherry said Kai’s doctor at UCHealth had to set up a special meeting to confirm the doctor could keep prescribing it.
So, for now, Kai has what he needs. But to Sherry, that is cold comfort.
“I don’t think that we are very safe,” she said. “These are just extensions.”
The family is coming up with a plan to leave the country. If Sherry and her husband can get jobs in New Zealand, they’ll move there. Sherry said such mobility is a privilege that many others don’t have.
For example, David, an 18-year-old student at Western Colorado University in the Rocky Mountain town of Gunnison. He asked to be identified only by his middle name because he worries he could be targeted in this conservative, rural town.
David doesn’t have a passport, but even if he did, he doesn’t want to leave Gunnison, he said. He is studying geology, is learning to play the bass, and has a good group of friends. He has plans to become a paleontologist.
His dorm room shelves are scattered with his essentials: fossils, Old Spice deodorant, microwave macaroni and cheese. But there are no mirrors. David said he got in the habit of avoiding them.
“For the longest time, I just had so much body dysphoria and dysmorphia that it can be kind of hard to look in the mirror,” David said. “But when I do, most of the time, I see something that I really like.”
He’s been taking testosterone for three years, and the hormone helped him grow a beard. In January, his doctor at Denver Health was told to stop prescribing it. His mom drove hours from her home to Gunnison to deliver the news in person.
That prescription is back on track now, but the mastectomy he’d planned for this summer isn’t. He’d hoped to have adequate recovery time before sophomore year. But he doesn’t know anyone in Colorado who would perform it until he is 19. He could easily get surgery to enhance his breasts, but he must seek surgical options in other states to reduce or remove them.
“Colorado as a state was supposed to be a safe haven,” said his mother, Louise, who asked to be identified by her middle name. “We have a law that makes it a right for trans people to have health care, and yet our health care systems are taking that away.”
It has taken eight years and about 10 medical providers and therapists to get David this close to the finish line. That’s a big deal after living through so many years of dysphoria and dysmorphia.
“I’m still going, and I’m going to keep going, and there’s almost nothing they can do to stop me — because this is who I am,” David said. “There have always been trans people, and there always will be trans people.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 months 1 week ago
california, Courts, Mental Health, Multimedia, States, Audio, Colorado, LGBTQ+ Health, Transgender Health, Trump Administration

Immigration Crackdowns Disrupt the Caregiving Industry. Families Pay the Price.
Alanys Ortiz reads Josephine Senek’s cues before she speaks. Josephine, who lives with a rare and debilitating genetic condition, fidgets her fingers when she’s tired and bites the air when something hurts.
Josephine, 16, has been diagnosed with tetrasomy 8p mosaicism, severe autism, severe obsessive-compulsive disorder, and attention-deficit/hyperactivity disorder, among other conditions, which will require constant assistance and supervision for the rest of her life.
Ortiz, 25, is Josephine’s caregiver. A Venezuelan immigrant, Ortiz helps Josephine eat, bathe, and perform other daily tasks that the teen cannot do alone at her home in West Orange, New Jersey. Over the past 2½ years, Ortiz said, she has developed an instinct for spotting potential triggers before they escalate. She closes doors and peels barcode stickers off apples to ease Josephine’s anxiety.
But Ortiz’s ability to work in the U.S. has been thrown into doubt by the Trump administration, which ordered an end to the temporary protected status program for some Venezuelans on April 7. On March 31, a federal judge paused the order, giving the administration a week to appeal. If the termination goes through, Ortiz would have to leave the country or risk detention and deportation.
“Our family would be gutted beyond belief,” said Krysta Senek, Josephine’s mother, who has been trying to win a reprieve for Ortiz.
Americans depend on many such foreign-born workers to help care for family members who are older, injured, or disabled and cannot care for themselves. Nearly 6 million people receive personal care in a private home or a group home, and about 2 million people use these services in a nursing home or other long-term care institution, according to a Congressional Budget Office analysis.
Increasingly, the workers who provide that care are immigrants such as Ortiz. The foreign-born share of nursing home workers rose three percentage points from 2007 to 2021, to about 18%, according to an analysis of census data by the Baker Institute for Public Policy at Rice University in Houston.
And foreign-born workers make up a high share of other direct care providers. More than 40% of home health aides, 28% of personal care workers, and 21% of nursing assistants were foreign-born in 2022, compared with 18% of workers overall that year, according to Bureau of Labor Statistics data.
That workforce is in jeopardy amid an immigration crackdown President Donald Trump launched on his first day back in office. He signed executive orders that expanded the use of deportations without a court hearing, suspended refugee resettlements, and more recently ended humanitarian parole programs for nationals of Cuba, Haiti, Nicaragua, and Venezuela.
In invoking the Alien Enemies Act to deport Venezuelans and attempting to revoke legal permanent residency for others, the Trump administration has sparked fear that even those who have followed the nation’s immigration rules could be targeted.
“There's just a general anxiety about what this could all mean, even if somebody is here legally,” said Katie Smith Sloan, president of LeadingAge, a nonprofit representing more than 5,000 nursing homes, assisted living facilities, and other services for aging patients. “There's concern about unfair targeting, unfair activity that could just create trauma, even if they don't ultimately end up being deported, and that's disruptive to a health care environment.”
Shutting down pathways for immigrants to work in the United States, Smith Sloan said, also means many other foreign workers may go instead to countries where they are welcomed and needed.
“We are in competition for the same pool of workers,” she said.
Growing Demand as Labor Pool Likely To Shrink
Demand for caregivers is predicted to surge in the U.S. as the youngest baby boomers reach retirement age, with the need for home health and personal care aides projected to grow about 21% over a decade, according to the Bureau of Labor Statistics. Those 820,000 additional positions represent the most of any occupation. The need for nursing assistants and orderlies also is projected to grow, by about 65,000 positions.
Caregiving is often low-paying and physically demanding work that doesn’t attract enough native-born Americans. The median pay ranges from about $34,000 to $38,000 a year, according to the Bureau of Labor Statistics.
Nursing homes, assisted living facilities, and home health agencies have long struggled with high turnover rates and staffing shortages, Smith Sloan said, and they now fear that Trump’s immigration policies will choke off a key source of workers, leaving many older and disabled Americans without someone to help them eat, dress, and perform daily activities.
With the Trump administration reorganizing the Administration for Community Living, which runs programs supporting older adults and people with disabilities, and Congress considering deep cuts to Medicaid, the largest payer for long-term care in the nation, the president’s anti-immigration policies are creating “a perfect storm” for a sector that has not recovered from the covid-19 pandemic, said Leslie Frane, an executive vice president of the Service Employees International Union, which represents nursing facility workers and home health aides.
The relationships caregivers build with their clients can take years to develop, Frane said, and replacements are already hard to find.
In September, LeadingAge called for the federal government to help the industry meet staffing needs by raising caps on work-related immigration visas, expanding refugee status to more people, and allowing immigrants to test for professional licenses in their native language, among other recommendations.
But, Smith Sloan said, “There's not a lot of appetite for our message right now.”
The White House did not respond to questions about how the administration would address the need for workers in long-term care. Spokesperson Kush Desai said the president was given “a resounding mandate from the American people to enforce our immigration laws and put Americans first” while building on the “progress made during the first Trump presidency to bolster our healthcare workforce and increase healthcare affordability.”
Refugees Fill Nursing Home Jobs in Wisconsin
Until Trump suspended the refugee resettlement program, some nursing homes in Wisconsin had partnered with local churches and job placement programs to hire foreign-born workers, said Robin Wolzenburg, a senior vice president for LeadingAge Wisconsin.
Many work in food service and housekeeping, roles that free up nurses and nursing assistants to work directly with patients. Wolzenburg said many immigrants are interested in direct care roles but take on ancillary roles because they cannot speak English fluently or lack U.S. certification.
Through a partnership with the Wisconsin health department and local schools, Wolzenburg said, nursing homes have begun to offer training in English, Spanish, and Hmong for immigrant workers to become direct care professionals. Wolzenburg said the group planned to roll out training in Swahili soon for Congolese women in the state.
Over the past 2½ years, she said, the partnership helped Wisconsin nursing homes fill more than two dozen jobs. Because refugee admissions are suspended, Wolzenburg said, resettlement agencies aren’t taking on new candidates and have paused job placements to nursing homes.
Many older and disabled immigrants who are permanent residents rely on foreign-born caregivers who speak their native language and know their customs. Frane with the SEIU noted that many members of San Francisco’s large Chinese American community want their aging parents to be cared for at home, preferably by someone who can speak the language.
“In California alone, we have members who speak 12 different languages,” Frane said. “That skill translates into a kind of care and connection with consumers that will be very difficult to replicate if the supply of immigrant caregivers is diminished.”
The Ecosystem a Caregiver Supports
Caregiving is the kind of work that makes other work possible, Frane said. Without outside caregivers, the lives of the patient and their loved ones become more difficult logistically and economically.
“Think of it like pulling out a Jenga stick from a Jenga pile, and the thing starts to topple,” she said.
Thanks to the one-on-one care from Ortiz, Josephine has learned to communicate when she’s hungry or needs help. She now picks up her clothes and is learning to do her own hair. With her anxiety more under control, the violent meltdowns that once marked her weeks have become far less frequent, Ortiz said.
“We live in Josephine’s world,” Ortiz said in Spanish. “I try to help her find her voice and communicate her feelings.”
Ortiz moved to New Jersey from Venezuela in 2022 as part of an au pair program that connects foreign-born workers with people who are older or children with disabilities who need a caregiver at home. Fearing political unrest and crime in her home country, she got temporary protected status when her visa expired last year to keep her authorization to work in the United States and stay with Josephine.
Losing Ortiz would upend Josephine’s progress, Senek said. The teen would lose not only a caregiver, but also a sister and her best friend. The emotional impact would be devastating.
“You have no way to explain to her, ‘Oh, Alanys is being kicked out of the country, and she can't come back,’” she said.
It’s not just Josephine: Senek and her husband depend on Ortiz so they can work full-time jobs and take care of themselves and their marriage. “She's not just an au pair,” Senek said.
The family has called its congressional representatives for help. Even a relative who voted for Trump sent a letter to the president asking him to reconsider his decision.
In the March 31 court decision, U.S. District Judge Edward Chen wrote that canceling the protection could “inflict irreparable harm on hundreds of thousands of persons whose lives, families, and livelihoods will be severely disrupted.”
‘Doing the Work That Their Own People Don’t Want To Do’
News of immigration dragnets that sweep up lawfully present immigrants and mass deportations are causing a lot of stress, even for those who have followed the rules, said Nelly Prieto, 62, who cares for an 88-year-old man with Alzheimer’s disease and a man in his 30s with Down syndrome in Yakima County, Washington.
Born in Mexico, she immigrated to the United States at age 12 and became a U.S. citizen under a law authorized by President Ronald Reagan that made any immigrant who entered the country before 1982 eligible for amnesty. So, she’s not worried for herself. But, she said, some of her co-workers working under H-2B visas are very afraid.
“It kills me to see them when they talk to me about things like that, the fear in their faces,” she said. “They even have letters, notarized letters, ready in case something like that happens, saying where their kids can go.”
Foreign-born home health workers feel they are contributing a valuable service to American society by caring for its most vulnerable, Prieto said. But their efforts are overshadowed by rhetoric and policies that make immigrants feel as if they don’t belong.
“If they cannot appreciate our work, if they cannot appreciate us taking care of their own parents, their own grandparents, their own children, then what else do they want?” she said. “We’re only doing the work that their own people don’t want to do.”
In New Jersey, Ortiz said life has not been the same since she received the news that her TPS authorization was slated to end soon. When she walks outside, she fears that immigration agents will detain her just because she’s from Venezuela.
She’s become extra cautious, always carrying proof that she’s authorized to work and live in the U.S.
Ortiz worries that she’ll end up in a detention center. But even if the U.S. now feels less welcoming, she said, going back to Venezuela is not a safe option.
“I might not mean anything to someone who supports deportations,” Ortiz said. “I know I'm important to three people who need me."
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 months 2 weeks ago
Aging, california, Health Care Costs, Health Industry, Multimedia, States, Audio, Disabilities, Home Health Care, Immigrants, Long-Term Care, New Jersey, Nursing Homes, Trump Administration, Wisconsin

Bird flu concerns mount as California reports more human cases
Concerns about bird flu — officially known as avian influenza A (H5) — continue to mount, particularly in California.
As of Oct. 14, the state has had six confirmed and five possible human cases of bird flu, according to the California Department of Public Health (CDPH).
All of the affected individuals reportedly had direct contact with infected cattle at nine dairy farms, the department stated.
FIRST CASE OF HUMAN BIRD FLU DIAGNOSED WITHOUT EXPOSURE TO INFECTED ANIMALS, CDC SAYS
The U.S. Centers for Disease Control and Prevention (CDC) is conducting tests to confirm the five possible cases.
All the individuals experienced "mild symptoms," including eye redness or discharge (conjunctivitis), the CDPH stated. None were hospitalized.
There is not a concern at this point about human-to-human transmission, according to the agency.
"Given the amount of exposure to infected cows, evidence continues to suggest only animal-to-human spread of the virus in California," said the CDPH statement.
"Additionally, based on CDC’s genomic sequencing of three California bird flu cases, there is no evidence to suggest an increased ability for the virus to infect or spread between people and no known reduced susceptibility to antiviral medications."
IN A POTENTIAL OUTBREAK, IS BIRD FLU TESTING AVAILABLE FOR HUMANS? WHAT TO KNOW
As of Oct. 15, there were a total of 20 confirmed human cases of bird flu in the U.S., according to the CDC.
Colorado and California have had the most cases, with others reported in Michigan, Missouri and Texas, the same source stated.
Roughly half of those were linked to exposure to infected cattle and the other half to infected poultry.
"To a large extent, the higher numbers we are seeing in California, and previously in Colorado, are due to more aggressive monitoring and case finding efforts in those states, rather than necessarily reflecting a larger burden of disease," Shira Doron, M.D., chief infection control officer at Tufts Medicine Health System in Boston, told Fox News Digital.
"California has one of the more comprehensive programs to find avian influenza in its cattle herds, and when they find sick cows, they monitor exposed farm workers," she went on.
"The disease has been mostly very mild, so it will only be detected if looked for."
It’s not known whether the strain that is causing avian flu in cows will ever mutate into a strain that can be spread from human to human, according to Doron.
"Right now, with no evidence of human-to-human spread, it does not have the potential to become a human pandemic, but that could change," she told Fox News Digital.
"Obviously, scientists and public health officials should be concerned, and should take action to limit the spread of this disease in farm animals."
BIRD FLU PANDEMIC IN FUTURE? EU WARNS OF POTENTIAL SPREAD TO HUMANS DUE TO 'LACK OF IMMUNE DEFENSE’
Farm owners and farm workers should also be concerned, she said.
"They should be taking measures to protect those who work closely with animals, especially cows and chickens," Doron advised.
Sam Scarpino, PhD, director of AI and life sciences at Northeastern University in Boston, said he finds the rising number of human H5N1 cases "concerning."
"The more spillovers to humans, the more chances there are for the wrong variant to find itself in a person and spark an epidemic," he told Fox News Digital.
There's currently no evidence, however, that the virus has mutated to become more infectious in humans, Scarpino said.
"Most likely, we are seeing the impact of an increasing number of infected dairy farms leading to an increasing number of human infections," he said.
"California also has active efforts for both human and dairy cattle surveillance, so ascertainment may be higher than in other states."
Although experts say the risk for human-to-human transmission remains low, they recommend certain public health precautions.
"People who have close contact with animals, particularly farm animals and wild birds, should be taking precautions," Doron advised.
CDC, WEBMD GIVE UPDATE ON CURRENT BIRD FLU OUTBREAK
The CDC also recommends that farm workers wear personal protective equipment — such as gloves, goggles and face shields — and that farms follow guidance to prevent the spread of the virus between animals.
"Even if a large outbreak isn't sparked, the risk to farm workers is clearly higher, and we need to ensure they are protected," Scarpino told Fox News Digital.
"At this point, there's no excuse for a farm worker to die from an H5N1 infection."
It’s also important for people to get their seasonal flu shot, experts say.
"While it is not likely to protect against avian flu, it will help people avoid being infected with the seasonal and avian strain at the same time, which can lead to genetic mixing and emergence of a pandemic strain," said Doron.
Getting the flu vaccine also makes it less likely that someone will end up with a suspected case of avian flu as a result of having the seasonal flu and a history of animal exposure, she added.
Vaccines for bird flu are currently in development.
"It is not time to vaccinate more broadly yet, given the small number of cases, absence of proven human-to-human transmission and mostly mild infection," said Doron.
It is important for tests to be commercially available for avian flu, however.
"Seasonal flu cases will be rising soon, and we will need to distinguish quickly between regular flu and avian flu, especially in animal workers," Doron noted.
CLICK HERE TO SIGN UP FOR OUR HEALTH NEWSLETTER
"Right now, to test for avian flu, specimens have to go to special public health labs and the results take days to return. We are going to need answers more quickly if we want people to be able to properly isolate and prevent spread."
The CDPH recommends that California residents monitor for bird flu symptoms for 10 days after exposure.
Those include eye redness (conjunctivitis), sore throat, cough, runny or stuffy nose, vomiting, diarrhea, muscle or body aches, fatigue, headaches, trouble breathing and fever.
For more Health articles, visit www.foxnews.com/health
"If they start to feel sick, they should immediately isolate, notify their local public health department, and work with public health and health care providers to get timely testing and treatment," the agency advises on its website.
9 months 1 week ago
Health, infectious-disease, viruses, cold-and-flu, mammals, birds, california, lifestyle