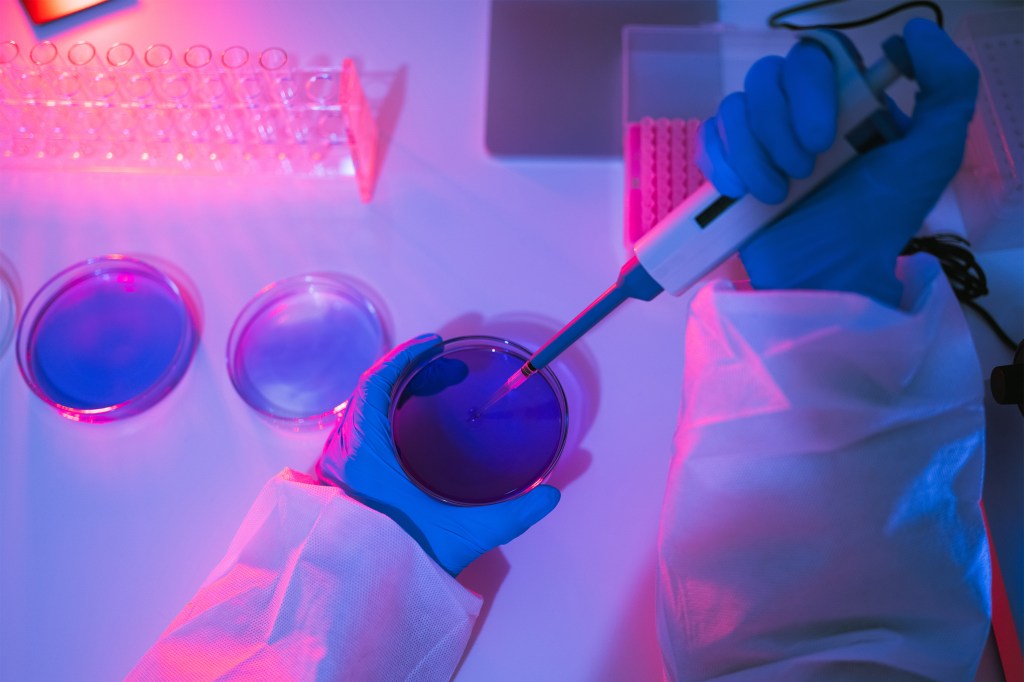
Beyond Ivy League, RFK Jr.’s NIH Slashed Science Funding Across States That Backed Trump
The National Institutes of Health’s sweeping cuts of grants that fund scientific research are inflicting pain almost universally across the U.S., including in most states that backed President Donald Trump in the 2024 election.
A KFF Health News analysis underscores that the terminations are sparing no part of the country, politically or geographically. About 40% of organizations whose grants the NIH cut in its first month of slashing, which started Feb. 28, are in states Trump won in November.
The Trump administration has singled out Ivy League universities including Columbia and Harvard for broad federal funding cuts. But the spending reductions at the NIH, the nation’s foremost source of funding for biomedical research, go much further: Of about 220 organizations that had grants terminated, at least 94 were public universities, including flagship state schools in places such as Florida, Georgia, Ohio, Nebraska, and Texas.
The Trump administration has canceled hundreds of grants supporting research on topics such as vaccination; diversity, equity, and inclusion; and the health of LGBTQ+ populations. Some of the terminations are a result of Trump’s executive orders to abandon federal work on diversity and equity issues. Others followed the Senate confirmation of anti-vaccine activist Robert F. Kennedy Jr. to lead the Department of Health and Human Services, which oversees the NIH. Many mirror the ambitions laid out in Project 2025’s “Mandate for Leadership,” the conservative playbook for Trump’s second term.
Affected researchers say Trump administration officials are taking a cudgel to efforts to improve the lives of people who often experience worse health outcomes — ignoring a scientific reality that diseases and other conditions do not affect all Americans equally.
KFF Health News found that the NIH terminated about 780 grants or parts of grants between Feb. 28 and March 28, based on documents published by the Department of Health and Human Services and a list maintained by academic researchers. Some grants were canceled in full, while in other cases, only supplements — extra funding related to the main grant, usually for a shorter-term, related project — were terminated.
Among U.S. recipients, 96 of the institutions that lost grants in the first month are in politically conservative states including Florida, Ohio, and Indiana, where Republicans control the state government or voters reliably support the GOP in presidential campaigns, or in purple states such as North Carolina, Michigan, and Pennsylvania that were presidential battleground states. An additional 124 institutions are in blue states.
Sybil Hosek, a research professor at the University of Illinois-Chicago, helps run a network that focuses on improving care for people 13 to 24 years old who are living with or at risk for HIV. The NIH awarded Florida State University $73 million to lead the HIV project.
“We never thought they would destroy an entire network dedicated to young Americans,” said Hosek, one of the principal investigators of the Adolescent Medicine Trials Network for HIV/AIDS Interventions. The termination “doesn’t make sense to us.”
NIH official Michelle Bulls is director of the Office of Policy for Extramural Research Administration, which oversees grants policy and compliance across NIH institutes. In terminating the grant March 21, Bulls wrote that research “based primarily on artificial and nonscientific categories, including amorphous equity objectives, are antithetical to the scientific inquiry, do nothing to expand our knowledge of living systems, provide low returns on investment, and ultimately do not enhance health, lengthen life, or reduce illness.”
Adolescents and young adults ages 13 to 24 accounted for 1 in 5 new HIV infections in the U.S. in 2022, according to the Centers for Disease Control and Prevention.
“It’s science in its highest form,” said Lisa Hightow-Weidman, a professor at Florida State University who co-leads the network. “I don’t think we can make America healthy again if we leave youth behind.”
HHS spokesperson Emily Hilliard said in an emailed statement that “NIH is taking action to terminate research funding that is not aligned with NIH and HHS priorities.” The NIH and the White House didn’t respond to requests for comment.
“As we begin to Make America Healthy Again, it's important to prioritize research that directly affects the health of Americans. We will leave no stone unturned in identifying the root causes of the chronic disease epidemic as part of our mission to Make America Healthy Again,” Hilliard said.
Harm to HIV, Vaccine Studies
The NIH, with its nearly $48 billion annual budget, is the largest public funder of biomedical research in the world, awarding nearly 59,000 grants in the 2023 fiscal year. The Trump administration has upended funding for projects that were already underway, stymied money for new applications, and sought to reduce how much recipients can spend on overhead expenses.
Those changes — plus the firing of 1,200 agency employees as part of mass layoffs across the government — are alarming scientists and NIH workers, who warn that they will undermine progress in combating diseases and other threats to the nation’s public health. On April 2, the American Public Health Association, Ibis Reproductive Health, and affected researchers, among others, filed a lawsuit in federal court against the NIH and HHS to halt the grant cancellations.
Two National Cancer Institute employees, who were granted anonymity because they were not authorized to speak to the press and feared retaliation, said its staff receives batches of grants to terminate almost daily. On Feb. 27, the cancer institute had more than 10,800 active projects, the highest share of the NIH’s roughly two dozen institutes and centers, according to the NIH’s website. At least 47 grants that NCI awarded were terminated in the first month.
Kennedy has said the NIH should take a years-long pause from funding infectious disease research. In November 2023, he told an anti-vaccine group, “I’m gonna say to NIH scientists, ‘God bless you all. Thank you for public service. We’re going to give infectious disease a break for about eight years,’” according to NBC News.
For years, Kennedy has peddled falsehoods about vaccines — including that “no vaccine” is “safe and effective,” and that “there are other studies out there” showing a connection between vaccines and autism, a link that has repeatedly been debunked — and claimed falsely that HIV is not the only cause of AIDS.
KFF Health News found that grants in blue states were disproportionately affected, making up roughly two-thirds of terminated grants, many of them at Columbia University. The university had more grants terminated than all organizations in politically red states combined. On April 4, Democratic attorneys general in 16 states sued HHS and the NIH to block the agency from canceling funds.
Researchers whose funding was stripped said they stopped clinical trials and other work on improving care for people with HIV, reducing vaping and smoking rates among LGBTQ+ teens and young adults, and increasing vaccination rates for young children. NIH grants routinely span several years.
For example, Hosek said that when the youth HIV/AIDS network’s funding was terminated, she and her colleagues were preparing to launch a clinical trial examining whether a particular antibiotic that is effective for men to prevent sexually transmitted infections would also work for women.
“This is a critically important health initiative focused on young women in the United States,” she said. “Without that study, women don’t have access to something that men have.”
Other scientists said they were testing how to improve health outcomes among newborns in rural areas with genetic abnormalities, or researching how to improve flu vaccination rates among Black children, who are more likely to be hospitalized and die from the virus than non-Hispanic white children.
“It's important for people to know that — if, you know, they are wondering if this is just a waste of time and money. No, no. It was a beautiful and rare thing that we did,” said Joshua Williams, a pediatric primary care doctor at Denver Health in Colorado who was researching whether sharing stories about harm experienced due to vaccine-preventable diseases — from missed birthdays to hospitalizations and job loss — might inspire caregivers to get their children vaccinated against the flu.
He and his colleagues had recruited 200 families, assembled a community advisory board to understand which vaccinations were top priorities, created short videos with people who had experienced vaccine-preventable illness, and texted those videos to half of the caregivers participating in the study.
They were just about to crack open the medical records and see if it had worked: Were the group who received the videos more likely to follow through on vaccinations for their children? That’s when he got the notice from the NIH.
“It is the policy of NIH not to prioritize research activities that focuses gaining scientific knowledge on why individuals are hesitant to be vaccinated and/or explore ways to improve vaccine interest and commitment,” the notice read.
Williams said the work was already having an impact as other institutions were using the idea to start projects related to cancer and dialysis.
A Hit to Rural Health
Congress previously tried to ensure that NIH grants also went to states that historically have had less success obtaining biomedical research funding from the government. Now those places aren’t immune to the NIH’s terminations.
Sophia Newcomer, an associate professor of public health at the University of Montana, said she had 18 months of work left on a study examining undervaccination among infants, which means they were late in receiving recommended childhood vaccines or didn’t receive the vaccines at all. Newcomer had been analyzing 10 years of CDC data about children’s vaccinations and had already found that most U.S. infants from 0 to 19 months old were not adequately vaccinated.
Her grant was terminated March 10, with the NIH letter stating the project “no longer effectuates agency priorities,” a phrase replicated in other termination letters KFF Health News has reviewed.
“States like Montana don’t get a lot of funding for health research, and health researchers in rural areas of the country are working on solutions to improve rural health care,” Newcomer said. “And so cuts like this really have an impact on the work we’re able to do.”
Montana is one of 23 states, along with Puerto Rico, that are eligible for the NIH’s Institutional Development Award program, meant to bolster NIH funding in states that historically have received less investment. Congress established the program in 1993.
The NIH’s grant terminations hit institutions in 15 of those states, more than half that qualify, plus Puerto Rico.
Researchers Can’t ‘Just Do It Again Later’
The NIH’s research funds are deeply entrenched in the U.S. health care system and academia. Rarely does an awarded grant stay within the four walls of a university that received it. One grant’s money is divvied up among other universities, hospitals, community nonprofits, and other government agencies, researchers said.
Erin Kahle, an infectious disease epidemiologist at the University of Michigan, said she was working with Emory University in Georgia and the CDC as part of her study. She was researching the impact of intimate partner violence on HIV treatment among men living with the virus. “They are relying on our funds, too,” she said.
Kahle said her top priority was to ethically and safely wind down her nationwide study, which included 418 people, half of whom were still participating when her grant was terminated in late March. Kahle said that includes providing resources to participants for whom sharing experiences of intimate partner violence may cause trauma or mental health distress.
Rachel Hess, the co-director of the Clinical & Translational Science Institute at the University of Utah, said the University of Nevada-Reno and Intermountain Health, one of the largest hospital systems in the West, had received funds from a $38 million grant that was awarded to the University of Utah and was terminated March 12.
The institute, which aims to make scientific research more efficient to speed up the availability of treatments for patients, supported over 5,000 projects last year, including 550 clinical trials with 7,000 participants. Hess said that, for example, the institute was helping design a multisite study involving people who have had heart attacks to figure out the ideal mix of medications “to keep them alive” before they get to the hospital, a challenge that’s more acute in rural communities.
After pushback from the university — the institute’s projects included work to reduce health care disparities between rural and urban areas — the NIH restored its grant March 29.
Among the people the Utah center thanked in its announcement about the reversal were the state’s congressional delegation, which consists entirely of Republican lawmakers. “We are grateful to University of Utah leadership, the University of Utah Board of Trustees, our legislative delegation, and the Utah community for their support,” it said.
Hilliard, of HHS, said that “some grants have been reinstated following the appeals process, and the agency will continue to carry out the remaining appeals as planned to determine their alignment.” She declined to say how many had been reinstated, or why the University of Utah grant was among them.
Other researchers haven’t had the same luck. Kahle, in Michigan, said projects like hers can take a dozen years from start to finish — applying for and receiving NIH funds, conducting the research, and completing follow-up work.
“Even if there are changes in the next administration, we’re looking at at least a decade of setting back the research,” Kahle said. “It’s not as easy as like, ‘OK, we’ll just do it again later.’ It doesn’t really work that way.”
Methodology
KFF Health News analyzed National Institutes of Health grant data to determine the states and organizations most affected by the Trump administration’s cuts.
We tallied the number of terminated NIH grants using two sources: a Department of Health and Human Services list of terminated grants published April 4; and a crowdsourced list maintained by Noam Ross of rOpenSci and Scott Delaney of the Harvard T.H. Chan School of Public Health, as of April 8. We focused on the first month of terminations: from Feb. 28 to March 28. We found that 780 awards were terminated in total, with 770 of them going to recipients based in U.S. states and two to recipients in Puerto Rico.
The analysis does not account for potential grant reinstatements, which we know happened in at least one instance.
Additional information on the recipients, such as location and business type, came from the USAspending.gov Award Data Archive.
There were 222 U.S. recipients in total. At least 94 of them were public higher education institutions. Forty-one percent of organizations that had NIH grants cut in the first month were in states that President Donald Trump won in the 2024 election.
Some recipients, including the University of Texas MD Anderson Cancer Center and Vanderbilt University Medical Center, are medical facilities associated with higher education institutions. We classified these as hospitals/medical centers.
We also wanted to see whether the grant cuts affected states across the political spectrum. We generally classified states as blue if Democrats control the state government or Democratic candidates won them in the last three presidential elections, and red if they followed this pattern but for Republicans. Purple states are generally presidential battleground states or those where voters regularly split their support between the two parties: Arizona, Michigan, Nevada, New Hampshire, North Carolina, Pennsylvania, Virginia, and Wisconsin. The result was 25 red states, 17 blue states, and eight purple states. The District of Columbia was also blue.
We found that, of affected U.S. institutions, 96 were in red or purple states and 124 were in blue states.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 months 1 week ago
Health Industry, Multimedia, Public Health, Race and Health, Rural Health, HIV/AIDS, Investigation, LGBTQ+ Health, Misinformation, NIH, Trump Administration, vaccines

Redadas contra inmigrantes afectan a la industria del cuidado. Las familias pagan el precio.
Alanys Ortiz entiende las señales de Josephine Senek antes de que ella pueda decir nada. Josephine, quien vive con una rara y debilitante condición genética, mueve los dedos cuando está cansada y muerde el aire cuando algo le duele.
Josephine tiene 16 años y ha sido diagnosticada con mosaicismo de tetrasomía 8p, autismo severo, trastorno obsesivo-compulsivo grave y trastorno por déficit de atención con hiperactividad, entre otras afecciones. Todo esto significa que necesitará asistencia y acompañamiento constantes toda su vida.
Ortiz, de 25 años, es la cuidadora de Josephine. Esta inmigrante venezolana la ayuda a comer, bañarse y hacer tareas diarias que la adolescente no puede hacer sola en su casa en West Orange, Nueva Jersey.
Ortiz cuenta que, en los últimos dos años y medio, ha desarrollado un instinto que le permite detectar posibles factores desencadenantes de las crisis antes de que se agudicen. Por ejemplo, cierra las puertas y les quita las etiquetas de códigos de barras a las manzanas para reducir la ansiedad de Josephine.
Sin embargo, la posibilidad de trabajar en Estados Unidos puede estar en peligro para Ortiz. La administración Trump ordenó poner fin al programa de Estatus de Protección Temporal (TPS) para algunos venezolanos a partir del 7 de abril. El 31 de marzo, un juez federal suspendió la orden, dando a la administración una semana para apelar.
Si el programa se suspende, Ortiz tendrá que abandonar el país o arriesgarse a ser detenida y deportada.
“Nuestra familia quedaría devastada más allá de lo imaginable”, afirma Krysta Senek, la madre de Josephine, quien ha estado buscando un indulto para Ortiz.
Los estadounidenses dependen de muchos trabajadores nacidos en el extranjero para cuidar a sus familiares mayores, lesionados o discapacitados que no pueden valerse por sí mismos.
Según un análisis de la Oficina de Presupuesto del Congreso, casi 6 millones de personas reciben atención personal en un hogar privado o en una residencia grupal, y alrededor de 2 millones utilizan estos servicios en residencias para personas mayores u otras instituciones de cuidado a largo plazo.
Cada vez con más frecuencia, estos cuidadores son inmigrantes como Ortiz. En los centros de cuidados para adultos mayores, la proporción de trabajadores nacidos en el extranjero aumentó tres puntos porcentuales entre 2007 y 2021, hasta alcanzar aproximadamente el 18%, según un análisis de datos del Censo del Instituto Baker de Política Pública de la Universidad Rice, en Houston.
Además, los trabajadores nacidos en el extranjero representan una gran parte de otros proveedores de cuidados directos.
En 2022, más del 40% de los asistentes de salud a domicilio, el 28% de los trabajadores de cuidado personal y el 21% de los asistentes de enfermería habían nacido en el extranjero, un número superior al 18% de extranjeros en el total de la economía ese año, según datos de la Oficina de Estadísticas Laborales.
Esa fuerza laboral está en riesgo como consecuencia de la ofensiva contra los inmigrantes que Donald Trump lanzó en el primer día de su segunda administración.
El presidente firmó órdenes ejecutivas que ampliaron los casos en los que se pueden decidir las deportaciones sin audiencia judicial, suspendieron los programas de reasentamiento de los refugiados y, más recientemente, pusieron fin a los programas de permiso humanitario para ciudadanos de Cuba, Haití, Nicaragua y Venezuela.
Recurriendo a la Ley de Enemigos Extranjeros para deportar a venezolanos e intentando revocar la residencia permanente de otros, la administración Trump ha generado temor incluso entre aquellos que han seguido las reglas de inmigración del país.
"Hay una ansiedad general sobre lo que esto podría significar, incluso si alguien está aquí legalmente", dijo Katie Smith Sloan, presidenta de LeadingAge, una organización sin fines de lucro que representa a más de 5.000 residencias, hogares de cuidados asistidos y otros servicios para adultos mayores.
“Existe preocupación por la persecución injusta, por acciones que pueden ser traumáticas incluso si finalmente esas personas no terminan siendo deportadas. Pero toda esa situación, ya de por sí, altera el entorno de atención de salud”.
Según explicó Smith Sloan, cerrar las vías legales para que los inmigrantes trabajen en Estados Unidos también implica que muchos optarán por irse a países donde sí son bienvenidos y necesarios.
“Estamos compitiendo por el mismo grupo de trabajadores”, afirmó.
Más demanda, menos trabajadores
Se prevé que la demanda de trabajadores que realizan tareas de cuidado aumente considerablemente en el país, a medida que los baby boomers más jóvenes lleguen a la edad de su jubilación.
Según las proyecciones de la Oficina de Estadísticas Laborales, la necesidad de asistentes de salud y de cuidado personal a domicilio crecerá hasta cerca del 21% en el transcurso de la próxima década.
Esos 820.000 puestos adicionales representan el mayor aumento entre todas las actividades laborales. También se proyecta un crecimiento en la demanda de auxiliares de enfermería y camilleros, con un incremento de alrededor de 65.000 puestos.
El trabajo de cuidado suele ser mal remunerado y físicamente exigente, por lo que en general no atrae a suficientes estadounidenses nativos. El salario medio oscila, según la misma Oficina, entre $34.000 y $38.000 anuales.
Los hogares para adultos mayores, las residencias geriátricas con asistencia y las agencias de atención domiciliaria han lidiado durante mucho tiempo con altas tasas de rotación de personal y escasez de empleados, señaló Smith Sloan.
Ahora, además, temen que las políticas migratorias de Trump corten una fuente clave de trabajadores, dejando a muchas personas de edad avanzada, o con discapacidades, sin alguien que las ayude a comer, a vestirse y a realizar sus actividades cotidianas.
Con el gobierno de Trump reorganizando la Administración para la Vida Comunitaria —encargada de los programas que apoyan a adultos mayores y personas con discapacidades— y el Congreso considerando recortes radicales a Medicaid (el mayor financiador de cuidados a largo plazo en el país), las políticas antiinmigración del presidente están generando “la tormenta perfecta” para un sector que aún no se ha recuperado de la pandemia de covid-19, opinó Leslie Frane, vicepresidenta ejecutiva del Sindicato Internacional de Empleados de Servicios, que representa a estos trabajadores.
Frane señaló que la relación que los cuidadores construyen con sus pacientes puede tardar años en desarrollarse, y que hoy ya es muy complicado encontrar personas que los reemplacen.
En septiembre, la organización LeadingAge hizo un llamado al gobierno federal para que ayudara a la industria a cubrir sus necesidades de personal. Le propuso, entre otras recomendaciones, que aumentara los cupos de visas de inmigración relacionadas con estos trabajos, ampliara el estatus de refugiado a más personas y permitiera que los inmigrantes rindieran los exámenes de certificación profesional en su idioma nativo.
Pero, agregó Smith Sloan, “en este momento no hay mucho interés en nuestro mensaje”.
La Casa Blanca no respondió a las preguntas sobre cómo la administración abordaría la necesidad de aumentar el número de trabajadores en el sector de cuidados a largo plazo.
El vocero Kush Desai declaró que el presidente recibió “un mandato contundente del pueblo estadounidense para hacer cumplir nuestras leyes migratorias y poner a los estadounidenses en primer lugar”, al tiempo que -dijo- continúa con “los avances logrados durante la primera presidencia de Trump para fortalecer al personal del sector salud y hacer que la atención médica sea más accesible”.
En Wisconsin, refugiados trabajan con adultos mayores
Hasta que Trump suspendió el programa de reasentamiento de refugiados, en Wisconsin algunas residencias de adultos mayores se habían asociado con iglesias locales y programas de inserción laboral para contratar trabajadores nacidos en el extranjero, explicó Robin Wolzenburg, vicepresidente senior de LeadingAge Wisconsin.
Muchas de estas personas trabajan en el servicio de comidas y en la limpieza, funciones que liberan a las enfermeras y auxiliares de enfermería para que puedan atender directamente a los pacientes.
Sin embargo, Wolzenburg agregó que muchos inmigrantes están interesados en asumir funciones de atención directa, pero que se emplean en funciones auxiliares porque no hablan inglés con fluidez o no tienen una certificación válida estadounidense.
Wolzenburg contó que, a través de una asociación con el departamento de salud de Wisconsin y las escuelas locales, los hogares de adultos mayores han comenzado a ofrecer formación en inglés, español y hmong para que los trabajadores inmigrantes puedan convertirse en profesionales de atención directa.
Dijo también que el grupo planeaba impartir pronto una capacitación en swahili para las mujeres congoleñas que viven en el estado.
En los últimos dos años y medio, esta colaboración ayudó a los centros de cuidados para personas mayores de Wisconsin a cubrir más de una veintena de puestos de trabajo, dijo.
Sin embargo, Wolzenburg explicó que, por la suspensión de las admisiones de refugiados, las agencias de reasentamiento no están incorporando nuevos candidatos y han puesto una pausa a la incorporación de estos trabajadores.
Muchos inmigrantes mayores o que tienen alguna discapacidad, y a la vez son residentes permanentes, dependen de cuidadores nacidos en el extranjero que hablen su idioma y conozcan sus costumbres.
Frane, del sindicato SEIU, señaló que muchos miembros de la numerosa comunidad chino-estadounidense de San Francisco quieren que sus padres mayores reciban atención en casa, preferiblemente de alguien que hable su mismo idioma.
“Solo en California, tenemos miembros del sindicato que hablan 12 lenguas diferentes, dijo Frane. Esa habilidad se traduce en una calidad de atención y una conexión con los usuarios que será muy difícil de replicar si disminuye la cantidad de cuidadores inmigrantes”.
El ecosistema que depende del trabajo de un cuidador
Las tareas de cuidado son el tipo de trabajo que permite que otros trabajos sean posibles, sostuvo Frane. Sin cuidadores externos, la vida de los pacientes y de sus seres queridos se vuelve más difícil desde el punto de vista logístico y económico.
“Es como sacar el pilar que sostiene todo lo demás: el sistema entero tambalea”, agregó.
Gracias a la atención personalizada de Ortiz, Josephine ha aprendido a comunicar cuando tiene hambre o necesita ayuda. Ahora recoge su ropa y está comenzando a peinarse sola. Como su ansiedad está más controlada, las crisis violentas que antes solían repetirse semana tras semana se han vuelto mucho menos frecuentes, dijo Ortiz.
"Vivimos en el mundo de Josephine", explica Ortiz en español. "Intento ayudarla a encontrar su voz y a expresar sus sentimientos".
Ortiz llegó a Nueva Jersey desde Venezuela en 2022 a través de un programa de Au Pair para conectar trabajadores nacidos en el extranjero con personas mayores o niños con discapacidades que necesitan cuidados en su hogar.
Temerosa de la inestabilidad política y la inseguridad en su país, cuando su visa expiró obtuvo el TPS el año pasado. Quería seguir trabajando en Estados Unidos, y quedarse con Josephine.
Perder a Ortiz sería un golpe devastador para el progreso de Josephine, aseguró Senek. La adolescente no solo se quedaría sin su cuidadora, sino también sin una hermana y su mejor amiga. El impacto emocional sería enorme.
"Nosotros no tenemos ninguna manera de explicarle a Josephine que Alanys está siendo expulsada del país y que no puede volver'", dijo Senek.
No se trata solo de Josephine: Senek y su esposo también dependen de Ortiz para poder trabajar a tiempo completo y cuidar de sí mismos y de su matrimonio. “Ella no es solo una Au Pair”, dijo Senek.
La familia ha contactado a sus representantes en el Congreso en busca de ayuda. Incluso un familiar que votó por Trump le envió una carta al presidente pidiéndole que reconsiderara su decisión.
En el fallo judicial del 31 de marzo, el juez federal Edward Chen escribió que cancelar esta protección podría “ocasionar un daño irreparable a cientos de miles de personas cuyas vidas, familias y medios de subsistencia se verán gravemente afectados”.
“Solo estamos haciendo el trabajo que su propia gente no quiere hacer”
Las noticias sobre redadas migratorias que detienen incluso a inmigrantes con estatus legal y las deportaciones masivas están generando mucho estrés, incluso entre quienes han seguido todas las reglas, comentó Nelly Prieto, de 62 años, quien cuida a un hombre de 88 con Alzheimer y a otro de unos 30 con síndrome de Down en el condado de Yakima, Washington.
Nacida en México, Prieto emigró a Estados Unidos a los 12 años y se convirtió en ciudadana estadounidense en virtud de una ley impulsada por el presidente Ronald Reagan que ofrecía amnistía a cualquier inmigrante que hubiera entrado en el país antes de 1982. Así que ella no está preocupada por sí misma. Pero, dijo, algunos de sus compañeros de trabajo con visados H-2B tienen mucho miedo.
“Me parte el alma verlos cuando me hablan de estas cosas, el miedo en sus rostros”, dijo. “Incluso tienen preparadas cartas firmadas ante un notario diciendo con quién deben quedarse sus hijos, por si algo llega a pasar”.
Los trabajadores de salud a domicilio que nacieron en el extranjero sienten que están contribuyendo con un servicio valioso a la sociedad estadounidense al cuidar de sus miembros más vulnerables, dijo Prieto. Pero sus esfuerzos se ven ensombrecidos por los discursos y las políticas que hacen que los inmigrantes se sientan como si fueran ajenos al país.
“Si no pueden apreciar nuestro trabajo, si no pueden apreciar que cuidemos de sus propios padres, de sus propios abuelos, de sus propios hijos, entonces, ¿qué más quieren?”, dijo. “Solo estamos haciendo el trabajo que su propia gente no quiere hacer”.
En Nueva Jersey, Ortiz contó que su vida no ha sido la misma desde que recibió la noticia de que su permiso bajo el TPS está por terminar. Cada vez que sale a la calle, teme que agentes de inmigración la detengan solo por ser venezolana.
Se ha vuelto mucho más precavida: siempre lleva consigo documentos que prueban que tiene autorización para vivir y trabajar en Estados Unidos.
Ortiz teme terminar en un centro de detención. Aunque Estados Unidos ahora no es un lugar acogedor, consideró que regresar a Venezuela no es una opción segura.
“Puede que yo no signifique nada para alguien que apoya las deportaciones”, dijo Ortiz. “Pero sé que soy importante para tres personas que me necesitan”.
Esta historia fue producida por Kaiser Health News, que publica California Healthline, un servicio editorialmente independiente de la California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 months 2 weeks ago
Aging, Health Care Costs, Health Industry, Noticias En Español, States, Disabilities, Home Health Care, Immigrants, Latinos, Long-Term Care, New Jersey, Washington
Immigration Crackdowns Disrupt the Caregiving Industry. Families Pay the Price.
Alanys Ortiz reads Josephine Senek’s cues before she speaks. Josephine, who lives with a rare and debilitating genetic condition, fidgets her fingers when she’s tired and bites the air when something hurts.
Josephine, 16, has been diagnosed with tetrasomy 8p mosaicism, severe autism, severe obsessive-compulsive disorder, and attention-deficit/hyperactivity disorder, among other conditions, which will require constant assistance and supervision for the rest of her life.
Ortiz, 25, is Josephine’s caregiver. A Venezuelan immigrant, Ortiz helps Josephine eat, bathe, and perform other daily tasks that the teen cannot do alone at her home in West Orange, New Jersey. Over the past 2½ years, Ortiz said, she has developed an instinct for spotting potential triggers before they escalate. She closes doors and peels barcode stickers off apples to ease Josephine’s anxiety.
But Ortiz’s ability to work in the U.S. has been thrown into doubt by the Trump administration, which ordered an end to the temporary protected status program for some Venezuelans on April 7. On March 31, a federal judge paused the order, giving the administration a week to appeal. If the termination goes through, Ortiz would have to leave the country or risk detention and deportation.
“Our family would be gutted beyond belief,” said Krysta Senek, Josephine’s mother, who has been trying to win a reprieve for Ortiz.
Americans depend on many such foreign-born workers to help care for family members who are older, injured, or disabled and cannot care for themselves. Nearly 6 million people receive personal care in a private home or a group home, and about 2 million people use these services in a nursing home or other long-term care institution, according to a Congressional Budget Office analysis.
Increasingly, the workers who provide that care are immigrants such as Ortiz. The foreign-born share of nursing home workers rose three percentage points from 2007 to 2021, to about 18%, according to an analysis of census data by the Baker Institute for Public Policy at Rice University in Houston.
And foreign-born workers make up a high share of other direct care providers. More than 40% of home health aides, 28% of personal care workers, and 21% of nursing assistants were foreign-born in 2022, compared with 18% of workers overall that year, according to Bureau of Labor Statistics data.
That workforce is in jeopardy amid an immigration crackdown President Donald Trump launched on his first day back in office. He signed executive orders that expanded the use of deportations without a court hearing, suspended refugee resettlements, and more recently ended humanitarian parole programs for nationals of Cuba, Haiti, Nicaragua, and Venezuela.
In invoking the Alien Enemies Act to deport Venezuelans and attempting to revoke legal permanent residency for others, the Trump administration has sparked fear that even those who have followed the nation’s immigration rules could be targeted.
“There's just a general anxiety about what this could all mean, even if somebody is here legally,” said Katie Smith Sloan, president of LeadingAge, a nonprofit representing more than 5,000 nursing homes, assisted living facilities, and other services for aging patients. “There's concern about unfair targeting, unfair activity that could just create trauma, even if they don't ultimately end up being deported, and that's disruptive to a health care environment.”
Shutting down pathways for immigrants to work in the United States, Smith Sloan said, also means many other foreign workers may go instead to countries where they are welcomed and needed.
“We are in competition for the same pool of workers,” she said.
Growing Demand as Labor Pool Likely To Shrink
Demand for caregivers is predicted to surge in the U.S. as the youngest baby boomers reach retirement age, with the need for home health and personal care aides projected to grow about 21% over a decade, according to the Bureau of Labor Statistics. Those 820,000 additional positions represent the most of any occupation. The need for nursing assistants and orderlies also is projected to grow, by about 65,000 positions.
Caregiving is often low-paying and physically demanding work that doesn’t attract enough native-born Americans. The median pay ranges from about $34,000 to $38,000 a year, according to the Bureau of Labor Statistics.
Nursing homes, assisted living facilities, and home health agencies have long struggled with high turnover rates and staffing shortages, Smith Sloan said, and they now fear that Trump’s immigration policies will choke off a key source of workers, leaving many older and disabled Americans without someone to help them eat, dress, and perform daily activities.
With the Trump administration reorganizing the Administration for Community Living, which runs programs supporting older adults and people with disabilities, and Congress considering deep cuts to Medicaid, the largest payer for long-term care in the nation, the president’s anti-immigration policies are creating “a perfect storm” for a sector that has not recovered from the covid-19 pandemic, said Leslie Frane, an executive vice president of the Service Employees International Union, which represents nursing facility workers and home health aides.
The relationships caregivers build with their clients can take years to develop, Frane said, and replacements are already hard to find.
In September, LeadingAge called for the federal government to help the industry meet staffing needs by raising caps on work-related immigration visas, expanding refugee status to more people, and allowing immigrants to test for professional licenses in their native language, among other recommendations.
But, Smith Sloan said, “There's not a lot of appetite for our message right now.”
The White House did not respond to questions about how the administration would address the need for workers in long-term care. Spokesperson Kush Desai said the president was given “a resounding mandate from the American people to enforce our immigration laws and put Americans first” while building on the “progress made during the first Trump presidency to bolster our healthcare workforce and increase healthcare affordability.”
Refugees Fill Nursing Home Jobs in Wisconsin
Until Trump suspended the refugee resettlement program, some nursing homes in Wisconsin had partnered with local churches and job placement programs to hire foreign-born workers, said Robin Wolzenburg, a senior vice president for LeadingAge Wisconsin.
Many work in food service and housekeeping, roles that free up nurses and nursing assistants to work directly with patients. Wolzenburg said many immigrants are interested in direct care roles but take on ancillary roles because they cannot speak English fluently or lack U.S. certification.
Through a partnership with the Wisconsin health department and local schools, Wolzenburg said, nursing homes have begun to offer training in English, Spanish, and Hmong for immigrant workers to become direct care professionals. Wolzenburg said the group planned to roll out training in Swahili soon for Congolese women in the state.
Over the past 2½ years, she said, the partnership helped Wisconsin nursing homes fill more than two dozen jobs. Because refugee admissions are suspended, Wolzenburg said, resettlement agencies aren’t taking on new candidates and have paused job placements to nursing homes.
Many older and disabled immigrants who are permanent residents rely on foreign-born caregivers who speak their native language and know their customs. Frane with the SEIU noted that many members of San Francisco’s large Chinese American community want their aging parents to be cared for at home, preferably by someone who can speak the language.
“In California alone, we have members who speak 12 different languages,” Frane said. “That skill translates into a kind of care and connection with consumers that will be very difficult to replicate if the supply of immigrant caregivers is diminished.”
The Ecosystem a Caregiver Supports
Caregiving is the kind of work that makes other work possible, Frane said. Without outside caregivers, the lives of the patient and their loved ones become more difficult logistically and economically.
“Think of it like pulling out a Jenga stick from a Jenga pile, and the thing starts to topple,” she said.
Thanks to the one-on-one care from Ortiz, Josephine has learned to communicate when she’s hungry or needs help. She now picks up her clothes and is learning to do her own hair. With her anxiety more under control, the violent meltdowns that once marked her weeks have become far less frequent, Ortiz said.
“We live in Josephine’s world,” Ortiz said in Spanish. “I try to help her find her voice and communicate her feelings.”
Ortiz moved to New Jersey from Venezuela in 2022 as part of an au pair program that connects foreign-born workers with people who are older or children with disabilities who need a caregiver at home. Fearing political unrest and crime in her home country, she got temporary protected status when her visa expired last year to keep her authorization to work in the United States and stay with Josephine.
Losing Ortiz would upend Josephine’s progress, Senek said. The teen would lose not only a caregiver, but also a sister and her best friend. The emotional impact would be devastating.
“You have no way to explain to her, ‘Oh, Alanys is being kicked out of the country, and she can't come back,’” she said.
It’s not just Josephine: Senek and her husband depend on Ortiz so they can work full-time jobs and take care of themselves and their marriage. “She's not just an au pair,” Senek said.
The family has called its congressional representatives for help. Even a relative who voted for Trump sent a letter to the president asking him to reconsider his decision.
In the March 31 court decision, U.S. District Judge Edward Chen wrote that canceling the protection could “inflict irreparable harm on hundreds of thousands of persons whose lives, families, and livelihoods will be severely disrupted.”
‘Doing the Work That Their Own People Don’t Want To Do’
News of immigration dragnets that sweep up lawfully present immigrants and mass deportations are causing a lot of stress, even for those who have followed the rules, said Nelly Prieto, 62, who cares for an 88-year-old man with Alzheimer’s disease and a man in his 30s with Down syndrome in Yakima County, Washington.
Born in Mexico, she immigrated to the United States at age 12 and became a U.S. citizen under a law authorized by President Ronald Reagan that made any immigrant who entered the country before 1982 eligible for amnesty. So, she’s not worried for herself. But, she said, some of her co-workers working under H-2B visas are very afraid.
“It kills me to see them when they talk to me about things like that, the fear in their faces,” she said. “They even have letters, notarized letters, ready in case something like that happens, saying where their kids can go.”
Foreign-born home health workers feel they are contributing a valuable service to American society by caring for its most vulnerable, Prieto said. But their efforts are overshadowed by rhetoric and policies that make immigrants feel as if they don’t belong.
“If they cannot appreciate our work, if they cannot appreciate us taking care of their own parents, their own grandparents, their own children, then what else do they want?” she said. “We’re only doing the work that their own people don’t want to do.”
In New Jersey, Ortiz said life has not been the same since she received the news that her TPS authorization was slated to end soon. When she walks outside, she fears that immigration agents will detain her just because she’s from Venezuela.
She’s become extra cautious, always carrying proof that she’s authorized to work and live in the U.S.
Ortiz worries that she’ll end up in a detention center. But even if the U.S. now feels less welcoming, she said, going back to Venezuela is not a safe option.
“I might not mean anything to someone who supports deportations,” Ortiz said. “I know I'm important to three people who need me."
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 months 2 weeks ago
Aging, california, Health Care Costs, Health Industry, Multimedia, States, Audio, Disabilities, Home Health Care, Immigrants, Long-Term Care, New Jersey, Nursing Homes, Trump Administration, Wisconsin

KFF Health News' 'What the Health?': The Ax Falls at HHS
The Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
As had been rumored for weeks, Health and Human Services Secretary Robert F. Kennedy Jr. unveiled a plan to reorganize the department. It involves the downsizing of its workforce, which formerly was roughly 80,000 people, by a quarter and consolidating dozens of agencies that were created and authorized by Congress.
Meanwhile, in just the past week, HHS abruptly cut off billions in funding to state and local public health departments, and canceled all research studies into covid-19, as well as diseases that could develop into the next pandemic.
This week’s panelists are Julie Rovner of KFF Health News, Maya Goldman of Axios News, Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico Magazine, and Alice Miranda Ollstein of Politico.
Panelists
Maya Goldman
Axios
Joanne Kenen
Johns Hopkins University and Politico
Alice Miranda Ollstein
Politico
Among the takeaways from this week’s episode:
- As federal health officials reveal the targets of a significant workforce purge and reorganization, the GOP-controlled Congress has been notably quiet about the Trump administration’s intrusions on its constitutional powers. Many of the administration’s attempts to revoke and reorganize federally funded work are underway despite Congress’ previous approval of that funding. And while changes might be warranted, reviewing how the federal government works (or doesn’t) — in the public forums of congressional hearings and floor debate — is part of Congress’ responsibilities.
- The news of a major reorganization at HHS also comes before the Senate finishes confirming its leadership team. New leaders of the National Institutes of Health and the FDA were confirmed just this week; Mehmet Oz, the nominated director of the Centers for Medicare & Medicaid Services, had not yet been confirmed when HHS made its announcement; and President Donald Trump only recently named a replacement nominee to lead the Centers for Disease Control and Prevention, after withdrawing his first pick.
- While changes early in Trump’s second term have targeted the federal government and workforce, the impacts continue to be felt far outside the nation’s capital. Indeed, cuts to jobs and funding touch every congressional district in the nation. They’re also being felt in research areas that the Trump administration claims as priorities, such as chronic disease: The administration said this week it will shutter the office devoted to studying long covid, a chronic disease that continues to undermine millions of Americans’ health.
- Meanwhile, in the states, doctors in Texas report a rise in cases of children with liver damage due to ingesting too much vitamin A — a supplement pushed by Kennedy in response to the measles outbreak. The governor of West Virginia signed a sweeping ban on food dyes and additives. And a woman in Georgia who experienced a miscarriage was arrested in connection with the improper disposal of fetal remains.
Also this week, Rovner interviews KFF senior vice president Larry Levitt about the 15th anniversary of the signing of the Affordable Care Act and the threats the health law continues to face.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week that they think you should read, too:
Julie Rovner: CNN’s “State Lawmakers Are Looking To Ban Non-Existent ‘Chemtrails.’ It Could Have Real-Life Side Effects,” by Ramishah Maruf and Brandon Miller.
Alice Miranda Ollstein: The New York Times Wirecutter’s “23andMe Just Filed for Bankruptcy. You Should Delete Your Data Now,” by Max Eddy.
Maya Goldman: KFF Health News’ “‘I Am Going Through Hell’: Job Loss, Mental Health, and the Fate of Federal Workers,” by Rachana Pradhan and Aneri Pattani.
Joanne Kenen: The Atlantic’s “America Is Done Pretending About Meat,” by Yasmin Tayag.
Also mentioned in this week’s podcast:
- The New York Times’ “West Virginia Bans 7 Artificial Food Dyes, Citing Health Concerns,” by Alice Callahan.
- The Washington Post’s “Why I Left My Job Leading Public Health Messaging for the CDC,” by Kevin Griffis.
- Politico’s “The Limits of RFK Jr.’s Power,” by Joanne Kenen.
Click to open the transcript
Transcript: The Ax Falls at HHS
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, March 27, at 10 a.m. As always, news happens fast — really fast this week — and things might well have changed by the time you hear this. So, here we go.
Today we are joined via videoconference by Alice Miranda Ollstein of Politico.
Alice Miranda Ollstein: Hello.
Rovner: Maya Goldman of Axios News.
Maya Goldman: Great to be here.
Rovner: And Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico Magazine.
Joanne Kenen: Hi everybody.
Rovner: Later in this episode we’ll have my interview with KFF Senior Vice President Larry Levitt, who will riff on the 15th anniversary of the signing of the Affordable Care Act and what its immediate future might hold. But first, this week’s news.
So for this second week in a row, we have news breaking literally as we sit down to tape, this time in the form of an announcement from the Department of Health and Human Services with the headline “HHS Announces Transformation to Make America Healthy Again.” The plan calls for 10,000 full-time employees to lose their jobs at HHS, and when combined with early retirement and other reductions, it will reduce the department’s workforce by roughly 25%, from about 82,000 to about 62,000. It calls for creation of a new “Administration for a Healthy America” that will combine a number of existing HHS agencies, including the Health Resources and Services Administration, the Agency for Toxic Substances and Disease Registry, and the National Institute for Occupational Safety and Health under one umbrella.
Reading through the announcement, a lot of it actually seems to make some sense, as many HHS programs do overlap. But the big overriding question is: Can they really do this? Isn’t this kind of reorganization Congress’ job?
Ollstein: Congress has not stood up for itself in its power-of-the-purse role so far in the Trump administration. They have stood by, largely, the Republican majorities in the House and Senate, or they’ve offered sort of mild concerns. But they have not said, Hey guys, this is our job, all of these cuts that are happening. There’s talk of a legislative package that would codify the DOGE [Department of Government Efficiency] cuts that are already happening, rubber-stamping it after the fact. But Congress has not made moves to claw back its authority in terms of saying, Hey, we approved this funding, and you can’t just go back and take it. There’s lawsuits to that effect, but not from the members — from outside groups, from labor unions, from impacted folks, but not our dear legislative branch.
Rovner: You know, Joanne, you were there for a lot of this. We covered the creation of a lot of these agencies. Agency for Healthcare Research and Quality, I covered the creation of its predecessor agency, which there were huge compromises that went into this, lots of policymaking. It just seems that RFK [Robert F. Kennedy] Jr. going to say: We don’t actually care all these things you did. We’re just going to redo the whole thing.
Kenen: As many of the listeners know, many laws that Congress passes have to be reauthorized every five years or every 10 years. Five is the most typical, and they often don’t get around to it and they extend and blah, blah, blah, blah, blah. But basically the idea is that things do change and things do need to be reevaluated. So, normally when you do reauthorization — we all just got this press release announcing all these mergers of departments and so forth at HHS. None of us are experts in procurement and IT. Maybe those two departments do need to be merged. I mean, I don’t know. That’s the kind of thing that, reauthorization, Congress looks at and Congress thinks about. Well, and agencies and legislation do get updated. Maybe the NIH [National Institutes of Health] doesn’t need 28 institutes and they should have 15 or whatever. But it’s just sort of this, somebody coming in and waving a magic DOGE wand, and Congress is not involved. And there’s not as much public input and expert input as you’d have because Congress holds hearings and listens to people who do have expertise.
So it’s not just Congress not exercising power to make decisions. It’s also Congress not deliberating and learning. I mean all of us learned health policy partly by listening to experts at congressional panels. We listen to people at Finance, and Energy and Commerce, and so forth. So it’s not just Congress’ voice being silenced. It’s this whole review and fact-based — and experts don’t always agree and Congress makes the final call. But that’s just been short-circuited. And I mean we all know there’s duplication in government, but this isn’t the process we have historically used to address it.
Rovner: You know, one other thing, I think they’re merging agencies that are in different locations, which on the one hand might make sense. But if you have one central IT or one central procurement agency in Washington or around Washington, you’ve got a lot of these organizations that are outside of Washington. And they’re outside of Washington because members of Congress put them there. A lot of them are in particular places because they were parochial decisions made by Congress. That may or may not make sense, but that’s where they are. It might or might not make sense. Maya, sorry I interrupted you.
Goldman: No, I was just going to add to Joanne’s point. Julie, I think before we started recording you mentioned that the administration is saying: We’ve thought this all out. These are well-researched decisions. But they’ve been in office for two months. How much research can you really do in that time and how intentional can those decisions really be in that time frame?
Ollstein: Especially because all of the leaders aren’t even in place yet. Some people were just confirmed, which we’re going to talk about. Some people are on their way to confirmation but not there yet. They haven’t had the chance to talk to career staff, figure out what the redundancies are, figure out what work is currently happening that would be disrupted by various closures and mergers and stuff. So Maya’s exactly right on that.
Goldman: You know there’s — the administration chose a lead for HRSA and other offices. And so what happens to those positions now? Do they just get demoted effectively because they’re no longer heads of offices? I would be pretty—
Rovner: But we have a secretary of education whose job is to close the department down, so—.
Goldman: Good point.
Rovner: That’s apparently not unprecedented in this administration. Well, as Alice was saying, into this maelstrom of change comes those that President [Donald] Trump has selected to lead these key federal health agencies. The Senate Tuesday night confirmed policy researcher Jay Bhattacharya to head the NIH and Johns Hopkins surgeon and policy analyst Marty Makary to head the Food and Drug Administration. Bhattacharya was approved on a straight party-line vote, while Makary, who I think it’s fair to say was probably the least controversial of the top HHS nominees, won the votes of three Democrats: Minority Whip Dick Durbin of Illinois and New Hampshire’s Democrats, [Sens.] Maggie Hassan and Jeanne Shaheen, along with all of the Republicans. What are any of you watching as these two people take up their new positions?
Kenen: Well, I mean, the NIH, Bhattacharya — who I hope I’ve learned to pronounce correctly and I apologize if I have not yet mastered it — he’s really always talked about major reorganization, reprioritization. And as I said, maybe it’s time to look at some overlap, and science has changed so much in the last decade or so. I mean are the 28 — I think the number’s 28 — are the 28 current institutes the right—
Rovner: I think it’s 27.
Kenen: Twenty-seven. I mean, are there some things that need to be merged or need to be reorganized? Probably. You could make a case for that. But that’s just one thing. The amount of cuts that the administration announced before he got there, and there is a question in some things he’s hinted at, is he going to go for that? His background is in academia, and he does have some understanding of what this money is used for. We’ve talked before, when you talk to a layperson, when you hear the word “overhead,” “indirect costs,” what that conjures up to people as waste, when in fact it’s like paying for the electricity, paying for the staff to comply with the government regulations about ethical research on human beings. It’s not parties. It’s security. It’s cleaning the animal cages. It’s all this stuff. So is he going to cut as deeply as universities have been told to expect? We don’t know yet. And that’s something that every research institution in America is looking at.
The FDA, he’s a contrarian on certain things but not across the board. I mean, as you just said, Julie, he’s a little less controversial than the others. He is a pancreatic surgeon. He does have a record as a physician. He has never been a regulator, and we don’t know exactly where his contrarian views will be unconventional and where — there’s a lot of agreement with certain things Secretary Kennedy wants to do, not everything. But there is some broad agreement on, some of his food issues do make sense. And the FDA will have a role in that.
Rovner: I will say that under this reorganization plan the FDA is going to lose 3,500 people, which is a big chunk of its workforce.
Kenen: Well things like moving SAMHSA [the Substance Abuse and Mental Health Services Administration], which is the agency that works on drug abuse within and drug addiction within HHS, that’s being folded into something else. And that’s been a national priority. The money was voted to help with addiction on a bipartisan basis several times in recent years. The grants to states, that’s all being cut back. The subagency with HHS is being folded into something else. And we don’t know. We know 20,000 jobs are being cut. The 10 announced today and the 10 we already knew about. We don’t know where they’re all coming from and what happens to the expertise and experience addressing something like the addiction crisis and the drug abuse crisis in America, which is not partisan.
Rovner: All right. Well we’ll get to the cuts in a second. Also on Tuesday, the Senate Finance Committee voted, also along party lines, to advance to the Senate floor the nomination of Dr. Mehmet Oz to head the Centers for Medicare & Medicaid Services. And while he would seem likely to get confirmed by the full Senate, I did not have on my bingo card Dr. Oz’s nomination being more in doubt due to Republicans than Democrats. Did anybody else?
Ollstein: Based on our reporting, it’s not really in doubt. [Sen.] Josh Hawley has raised concerns about Dr. Oz being too squishy on abortion and trans health care, but it does not seem that other Republicans are really jumping on board with that crusade. It sort of reminds me of concerns that were raised about RFK Jr.’s background on abortion that pretty much just fizzled and Republicans overwhelmingly fell in line. And that seems to be what’s going to happen now. Although you never know.
Rovner: At least it hasn’t been, as you point out, it hasn’t failed anybody else. Well, the one nominee who did not make it through HHS was former Congressman Dave Weldon to head the CDC [Centers for Disease Control and Prevention]. So now we have a new nominee. It’s actually the acting director, Susan Monarez, who by the way has a long history in federal health programs but no history at the CDC. Who can tell us anything about her?
Goldman: She seems like a very interesting and in some ways unconventional pick, especially for this administration. She was a career civil servant, and she worked under the Obama administration. And it’s interesting to see them be OK with that, I think. And she also has a lot of health care background but not in CDC. She’s done a lot of work on AI in health care and disaster preparedness, I think. And clearly she’s been leading the CDC for the last couple months. So she knows to that extent. But it will be very interesting when she gets around to confirmation hearings to hear what her priorities are, because we really have no idea.
Rovner: Yeah, she’s not one of those good-on-Fox News people that we’ve seen so many of in this administration. So while Monarez’s nomination seems fairly noncontroversial, at least so far, the nominee to be the new HHS inspector general is definitely not. Remember that President Trump fired HHS IG Christi Grimm just days after he took office, along with the IGs of several other departments. Grimm is still suing to get her job back, since that firing violated the terms of the 1978 Inspector General Act. But now the administration wants to replace her with Thomas Bell, who’s had a number of partisan Republican jobs for what’s traditionally been a very nonpartisan position and who was fired by the state of Virginia in 1997 for apparently mishandling state taxpayer funds. That feels like it might raise some eyebrows as somebody who’s supposed to be in charge of waste, fraud, and abuse. Or am I being naive?
Goldman: My eyebrows were definitely raised when I saw that news. I, to be honest, don’t know very much about him but will be very interested to see how things go, especially given that fraud, waste, and abuse and rooting out fraud, waste, and abuse are high priorities for this administration, but also things that are very up to interpretation in a certain way.
Ollstein: Yes, although it’s clearly been very mixed on that front because the administration is also dismantling entire agencies that go after fraud and abuse—
Goldman: Exactly.
Ollstein: —like the Consumer Financial Protection Bureau. So there is some mixed messaging on that front for sure.
Rovner: Well, as Joanne mentioned, the DOGE cuts continue at the NIH. In just the last week, billions of dollars in grants have been terminated that were being used to study AIDS and HIV, covid and other potential pandemic viruses, and climate change, among other things. The NIH also closed its office studying long covid. Thank you, Alice, for writing that story. This is, I repeat, not normal. NIH only generally cancels grants that have been peer reviewed and approved for reasons of fraud or scientific misconduct, yet one termination letter obtained by Science Magazine simply stated, quote, “The end of the pandemic provides cause to terminate COVID-related grant funds.” Why aren’t we hearing more about this, particularly for members of Congress whose universities are the ones that are being cut?
Kenen: I mean, the one Republican we heard at the very beginning was [Sen.] Katie Britt because the University of Alabama is a big, excellent, and well-respected national medical and science center, and they were targeted for a lot of cuts. She’s the only Republican, really, and she got quiet. I mean, she raised her voice very loud and clear. We may go into a situation — and everybody sort of knows this is how Washington sometimes works — where individual universities will end up negotiating with NIH over their funds and that—
Rovner: Columbia. Cough, cough.
Kenen: Right. And Alabama may come out great and Columbia might not, or many other leading research institutions. But these job cuts affect people in every congressional district across the country. And the funding cuts affect every congressional district across the country. So it’s not just their constitutional responsibilities. It’s also, like, their constituents are affected, and we’re not hearing it.
Rovner: And as I point out for the millionth time, it’s not a coincidence that these things are located in every congressional district. Members of Congress, if not the ones who are currently in office then their predecessors, lobbied and worked to get these funds to their states and to their district. And yet the silence is deafening.
Ollstein: To state the obvious, one, covid is not over. People are still contracting it. People are still dying from it. But not only that, a lot of this research was about preparing for the inevitable next pandemic that we know is coming at some point and to not be caught as unawares as we were this past time, to be more prepared, to have better tools so that there don’t have to be widespread lockdowns, things can remain open because we have more effective prevention and treatment efforts. And that’s what’s being defunded here.
Kenen: The other thing is that long covid is in fact a chronic disease and even though it’s caused by an infectious disease, a virus. But people have long covid but it is a chronic disease, and HHS says that’s their priority, chronic disease, but they’re not including long covid. And there’s also more and more. When we think of long covid, we think of brain fog and being short of breath and tired and unable to function. There’s increasing evidence or conversation in the medical world about other problems people have long-term that probably stem from covid infections or multiple covid infections. So this is affecting millions of Americans as a chronic disease that is not well understood, and we’ve just basically said, That one doesn’t count, or: We’re not going to pay attention to that one. We’re going to, you know, we’re looking at diabetes. Yeah, we need to look at diabetes. That’s one of the things that Kennedy has bipartisan support. This country does not eat well. I wrote about this about a week ago. But what he can and can’t do, because he can’t wave a magic wand and have us all eating well. But it’s very selective in how we’re defining both the causes of diseases and what diseases we’re prioritizing. We basically just shrunk addiction.
Goldman: In the press release announcing the reorganization this morning, there was a line talking about how the HHS is going to create this new Administration for a Healthy America to investigate chronic disease and to make sure that we have, I think it was, wholesome food, clean water, and no environmental toxins, in order to prevent chronic disease. And those are the only three things that it mentions that lead to chronic disease.
Rovner: And none of which are under HHS’ purview.
Goldman: Right, right. Yeah.
Rovner: With the exception of—
Goldman: There are things that HHS does in that space. But yeah, we’re being very selective about what constitutes a chronic disease and what causes a chronic disease. If you’re trying to actually solve a problem, maybe you should be more expansive.
Kenen: So HHS has some authority over food, not significant authority of it, but it is shared with the USDA [U.S. Department of Agriculture]. Like school lunches are USDA, the nutritional guidelines are shared between USDA and HHS, things like that. So yeah, it has some control about, over food but not entirely control over food.
And then EPA [Environmental Protection Agency], which has also been completely reoriented to be a pro-fossil-fuel agency, is in charge of clean water and the environmental contaminants. That’s not an HHS bailiwick. And Kennedy is not aligned with other elements of the administration on environmental issues. And also genetics, right? Genetics is also, you know, who knows? That’s NIH? But who knows what’s going to happen to the National Cancer Institute and other genetic research at NIH? We don’t know.
Rovner: Yes. Clearly much to be determined. Well, speaking of members of Congress whose states and districts are losing federal funds, federal aid is also being cut by the CDC. In a story first reported by NBC News, CDC is reportedly clawing back more than $11 billion in covid-related grants. Among other things, that’s impacting funding that was being used in Texas to fight the ongoing measles outbreak. How exactly does clawing back this money from state and local public health agencies make America healthy again?
Goldman: That’s a great question, and I’m curious to see how it plays out. I don’t have the answer.
Rovner: And it’s not just domestic spending. The fate of PEPFAR [the President’s Emergency Plan for AIDS Relief], the international AIDS/HIV program that’s credited with saving more than 20 million lives, remains in question. And The New York Times has gotten hold of a spreadsheet including more global health cuts, including those for projects to fight malaria and to pull the U.S. out of Gavi. That’s the global vaccine alliance that’s helped vaccinate more than 1.1 billion children in 78 countries. Wasn’t there a court order stopping all of these cuts?
Ollstein: So there was for some USAID [U.S. Agency for International Development] work, but not all of these things fall under that umbrella. And that is still an ongoing saga that has flipped back and forth depending on various rulings. But I think it’s worth pointing out, as always, that infectious diseases don’t respect international borders, and any pullback on efforts to fight various things abroad inevitably will impact Americans as well.
Rovner: Yeah. I mean, we’ve seen these measles cases obviously in Texas, but now we’re getting measles cases in other parts of the country, and many of them are people coming from other countries. We had somebody come through Washington, D.C.’s Union Station with measles, and we’ve had all of these alerts. I mean, this is what happens when you don’t try and work with infectious diseases where they are, then they spread. That’s kind of the nature of infectious disease.
Well, at the same time, HHS Secretary RFK Jr. is putting his Make America Healthy Again agenda into practice in smaller ways as well. First up, remember that study that Kennedy promised again to look into any links between childhood vaccines and autism? It will reportedly be led by a vaccine skeptic who was disciplined by the Maryland Board of Physicians for practicing medicine without a license and who has pushed the repeatedly debunked assertion that autism can be caused by the preservative thimerosal, which used to be used in childhood vaccines but has long since been discontinued. One autism group referred to the person who’s going to be running this study as, quote, “a known conspiracy theorist and quack.” Sen. [Bill] Cassidy seemed to promise us that this wasn’t going to happen.
Kenen: Well, we think that Sen. Cassidy was promised it wouldn’t happen, and it’s all happening. And in fact, when a recent hearing, he was very outspoken that there’s no need to research the autism link, because it’s been researched over and over and over and over and over again and there’s a lot of reputable scientific evidence establishing that vaccination does not cause autism. We don’t know what causes autism, so—
Rovner: But we know it’s not thimerosal.
Kenen: Right, which has been removed from many vaccines, in fact, and autism rates went up. So Cassidy has not come out and said, Yeah, I’m the guy who pulled the plug on Weldon. But it’s sort of obvious that he had, at least was, a role in. It is widely understood in Washington that he and a few other Republicans, [Sens. Lisa] Murkowski and [Susan] Collins, I believe — I think Murkowski said it in public — said that the CDC could not go down that route.
Rovner: Well, I would like to be inadvertently invited to the Signal chat between Secretary Kennedy and Sen. Cassidy. I would very much wish to see that conversation.
Meanwhile, in Texas, where HHS just confiscated public health funding, as we said, a hospital in Lubbock says it’s now treating children with liver damage from too much vitamin A, which Secretary Kennedy recommended as a way to prevent and or treat measles. Which it doesn’t, by the way. But that points to, that some of these — I hesitate of how to describe these people who are “making America healthy again.” But some of the things that they point to can be actively dangerous, not just not helpful.
Goldman: Yeah. And I think it also shows how much messaging from the top matters, right? People are listening to what Secretary Kennedy says, which makes sense because he’s the secretary of health and human services. But if he’s pedaling misinformation or disinformation, that can have real harmful effects on people.
Kenen: And his messages are being amplified even if some people are not, their parents, who aren’t maybe directly tuned in to what Kennedy personally is saying, but they follow various influencers on health who are then echoing what Kennedy’s saying about vitamin A. Yeah, we all need vitamin A in our diet. It’s something, part of healthy nutrition. But this supplement’s unnecessary, or excess supplements, vitamin A or cod liver oil or other things that can make them sick, including liver damage. And that’s what we’re seeing now. Vitamin A does have a place in measles under very specific circumstances, under medical supervision in individual cases. But no, people should not be going to the drugstore and pouring huge numbers of tablets of vitamin C down their children’s throat. It’s dangerous.
Rovner: And actually the head of communications at the CDC not only quit his job this week but wrote a rather impassioned op-ed in The Washington Post, which I will post in our show notes, talking about he feels like he cannot work for an agency that is not giving advice that is based in science and that that’s what he feels right now. Again, that’s before we get a new head of the CDC. Well, MAHA is apparently spreading to the states as well. West Virginia Republican Gov. Patrick Morrisey this week signed a bill to ban most artificial food coloring and two preservatives in all foods sold in the state starting in 2028. Nearly half the rest of the states are considering similar types of bans. But unless most of those other states follow, companies aren’t going to remake their products just for West Virginia, right?
Kenen: West Virginia is not big enough, but they sometimes do remake their products for California, which is big. The whole food additive issue is, traditionally the food manufacturers have had a lot of control over deciding what’s safe. It’s the industry that has decided. Kennedy has some support across the board and saying that’s too loose and we should look at some of these additives that have not been examined. There are others, including some preservatives, that have been studied and that are safe. Some preservatives have not been studied and should be studied. There are others that have been studied and are safe and they keep food from going rotten or they can prevent foodborne disease outbreaks. Something that does make our food healthy, we probably want to keep them in there. So, and are there some that—
Rovner: I think people get mixed up between the dyes and the preservatives. Dyes are just to make things look more attractive. The preservatives were put there for a reason.
Kenen: Right. And there’s some healthy ways of making dyes, too, if you need your food to be red. There’s berry abstracts instead of chemical extracts. So things get overly simplified in a way that does not end up necessarily promoting health across the board.
Rovner: Well, not all of the news is coming from the Trump administration. The Supreme Court next week will hear a case out of South Carolina about whether Medicaid recipients can sue to enforce their right to get care from any qualified health care providers. But this is really another case about Planned Parenthood, right, Alice?
Ollstein: Yep. If South Carolina gets the green light to kick Planned Parenthood out of its Medicaid program, which is really what is at the heart of this case, even though it’s sort of about whether beneficiaries can sue if their rights are denied. A right isn’t a right if you can’t enforce it, so it’s expected that a ruling in that direction would cause a stampede of other conservative states to do the same, to exclude Planned Parenthood from their Medicaid programs. Many have tried already, and that’s gone around and around in the courts for a while, and so this is really the big showdown at the high court to really decide this.
And as I’ve been writing about, this is just one of many prongs of the right’s bigger strategy to defund Planned Parenthood. So there are efforts at the federal level. There are efforts at the state level. There are efforts in the courts. They are pushing executive actions on that front. We can talk. There was some news on Title X this week.
Rovner: That was my next question. Go ahead.
Ollstein: Some potential news.
Rovner: What’s happening with Title X?
Ollstein: Yeah. So HHS told us when we inquired that nothing’s final yet, but they’re reviewing tens of millions of Title X federal family planning grants that currently go to some Planned Parenthood affiliates to provide subsidized contraception, STI [sexually transmitted infection] screenings, various non-abortion services. And so they are reviewing those grants now. They are supposed to be going out next week, so we’ll have to see what happens there. There was some sort of back-and-forth in the reporting about whether they’re going to be cut or not.
Rovner: What surprises me about the Title X grant, and there has been, there have been efforts, as you point out, going back to the 1980s to kick Planned Parenthood out of the Title X program. That’s separate from kicking Planned Parenthood out of Medicaid, which is where Planned Parenthood gets a lot more money.
But the first Trump administration did kick Planned Parenthood out of Title X, and they went through the regulatory process to do it. And then the Biden administration went through the regulatory process to rescind the Trump administration regulations that kicked them out. Now it looks like the Trump administration thinks that it can just stop it without going through the regulatory process, right?
Ollstein: That’s right. So not only are they going around Congress, which approves Title X funding every year, they are also going around their own rulemaking and just going for it. Although, again, it has not been finally announced whether or not there will be cuts. They’re just reviewing these grants.
Rovner: But I repeat for those in the back, this is not normal. It’s not how these things are supposed to work it.
Kenen: It’s normal now, Julie.
Rovner: Yeah, clearly it’s becoming normal. Well, finally this week, another case of a woman arrested for a poor pregnancy outcome. This happened in Georgia where the woman suffered a natural miscarriage, not an abortion, which was confirmed by the medical examiner, but has been arrested on charges of improperly disposing of the fetal remains. Alice, this is turning into a trend, right?
Ollstein: Yes. And it’s important for people to remember that this was happening before Dobbs. This was happening when Roe v. Wade was still in place. This has happened since then in states where abortion is legal. Some prosecutors are finding other ways to charge people. Whether it’s related to, yeah, the disposal of the fetus, whether it’s related to substance abuse, substance use during pregnancy, even sometimes the use of substances that are actually legal, but people have been charged, arrested for using them during pregnancy. So yes, it’s important to remember that even if there’s not a quote-unquote “abortion ban” on the books, there are still efforts underway in many places to criminalize pregnancy loss however it happens, naturally or via some abortifacient method.
Rovner: Well, something else we’ll be keeping an eye on. All right, that’s as much news as we have time for this week. Now, we will play my interview with KFF’s Larry Levitt. Then we’ll come back and do our extra credits.
So, last Sunday was the 15th anniversary of President Barack Obama’s signing of the original Affordable Care Act. And before you ask, yes, I was there in the White House East Room that day. Anyway, to discuss what the law has meant to the U.S. health system over the last decade and a half and what its future might be, I am so pleased to welcome back to the podcast my KFF colleague Larry Levitt, executive vice president for health policy.
Larry, thanks for joining us again.
Larry Levitt: Oh, thanks for having me.
Rovner: So, [then-House Speaker] Nancy Pelosi was mercilessly derided when she said that once the American people learned exactly what was in the ACA, they would come to like it. But that’s exactly what’s happened, right?
Levitt: It is. Yes. I think people took her comments so out of context, but the ACA was incredibly controversial and divisive when it was being debated. Frankly, after a pass, the ACA became pretty unpopular. If you go back to 2014, just before the main provisions of the ACA were being implemented, there was all this controversy over the individual mandate, over people’s plans being canceled because they didn’t comply with the ACA’s rules. And then, of course, healthcare.gov, the website, didn’t work. So the ACA was very underwater in public opinion. And even after it first went into effect and people started getting coverage, that didn’t necessarily turn around immediately, there was still a lot of divisiveness over the law.
What changed is, No. 1, over time, more and more people got covered, people with preexisting conditions, people who couldn’t afford health insurance, people who turned 26 or could stay on their parents’ plans until 26 and then could enroll in the ACA or Medicaid after turning 26. All these people got coverage and started to see the benefits of the law. The other thing that happened was in 2017, Republicans tried unsuccessfully to repeal and replace the ACA, and people really realized what they could be missing if the law went away.
Rovner: So what’s turned out to be the biggest change to the health care system as a result of the ACA? And is it what you originally thought it would be?
Levitt: Well, yeah, in this case it was not a surprise, I think. The biggest change was the number of people getting covered and a big decrease in the number of people uninsured. We have been at the lowest rate of uninsurance ever recently due to the ACA and some of the enhancements, which we’ll probably talk about. And that was what the law was intended to do, was to get more people covered. And I think you’d have to call that a success, in retrospect.
Rovner: I will say I was surprised by how much Medicaid dominated the increased coverage. I know now it’s sort of balanced out because of reductions in premiums for private coverage, I think in large part. But I think during the 2017 fight to undo the ACA, that was the first time since I’ve been covering Medicaid that I think people really realized how big and how important Medicaid is to the health care system.
Levitt: No, that’s right. I mean the ACA marketplace, healthcare.gov, the individual mandate, preexisting condition protections, I mean, those are the things that got a lot of the public attention. But in fact, yeah, in the early years of the ACA, I mean really up until just the last couple years, the Medicaid expansion in the ACA was really the engine of coverage. And that’s not what a lot of people expected. In fact, Congressional Budget Office in their original projections kind of got that wrong, too.
Rovner: So what was the biggest disappointment about something the ACA was supposed to do but didn’t do or didn’t do very well?
Levitt: Yeah, I mean, I would have to point to health care costs as the biggest disappointment. The ACA really wasn’t intended to address health care costs head-on. And that was both a policy judgment but also a political decision. If you go back to the debate over the Clinton health plan in the early ’90s, which failed spectacularly — you and I were both there — it addressed health care costs aggressively, took on every segment of the health care industry, and died under that political weight. The political judgment of Obama and Democrats in Congress with the ACA was to not take on those vested health care interests and not really address health care costs head-on. That’s what enabled it to get passed. But it sort of lacked teeth in that regard. There were some things in the ACA like expansion of ACOs, accountable care organizations, which maybe had some promise but frankly have not done a whole lot.
Rovner: And of course, Congress undoing what teeth there were in the ensuing years probably didn’t help very much, either.
Levitt: No. I mean there was this provision in the ACA called the Cadillac plan tax, right? The idea was to tax so-called Cadillac health plans, very generous health plans. That probably would’ve had an effect. I’m not sure it would’ve done what people intended for it to do. I mean, I think it would’ve actually shifted costs to workers and caused deductibles to rise even higher. But no one but economists liked that Cadillac plan tax, and it was repealed.
Rovner: So, as you mentioned, you and I are both also veterans of the 1993, 1994 failed effort by President Bill Clinton to overhaul the nation’s health care system, which, like the fight over the ACA, featured large-scale, deliberate mis- and disinformation by opponents about what a major piece of health legislation could do. In fact, and I have done lots of stories on this, scare tactics about the possible impact of providing universal health insurance coverage date back to the early 1900s and have been a feature of every single major health care debate since then. What did we learn from the ACA debate about combating this kind of deliberate misinformation?
Levitt: Yeah, you’re so right about the disinformation, and I was actually looking yesterday — we have a timeline of health policy over the decades in our KFF headquarters in San Francisco, and we have an ad up there from the debate over the Truman health plan. You and I were not there for that debate.
Rovner: Thank you.
Levitt: And the AMA [American Medical Association] opposed that as socialized medicine and ran these ads featuring robots who were going to be your doctor if the Truman plan passed. So this is certainly nothing new. And we saw it in the ACA with death panels, right? I mean, which just spread like wildfire through the media and over social media. I would kind of hope we learned some lessons from the ACA. I’m not sure we have. And I kind of worry that with declining trust in institutions, particularly government institutions, I just wonder whether we’ll get back to a place where, yeah, we’ll disagree about policy. There will be spin, there will be scare tactics, but at least there’s some trusted source of facts and data that we can rely on, and I’m not so hopeful there.
Rovner: Somebody asked former [HHS] Secretary Kathleen Sebelius at a 15th-anniversary event what she regretted most about not having in the ACA, and she said, With all the talk of our actually taking over the health care system, we should have just taken over the health care system, since that’s what everybody was accusing it of. It might’ve worked better.
Levitt: Yeah, there is — we could have a whole other session on “Medicare for All” and single payer and the pros and cons of that. But one thing I think we did learn from the ACA, that complexity is just a huge problem. Even what’s supposed to be the simplest part of our health care system now, Medicare, has become incredibly complex with Part A and Part B and Part C and Part D. Seniors kind of scratch their heads trying to figure out what to do, and the ACA even more so.
And I think back to your original question, part of what made the ACA so hard for people to grasp is there was not one single, Oh, I’m going to sign up for the ACA. There were so many pieces of it. And over time, I’m not even sure people identify those pieces with the ACA anymore.
Rovner: Yeah. Oh, no, I am surprised at how many younger people have no idea of what the insurance market was like before the ACA and how many people were simply redlined out of getting coverage.
Levitt: Right. No. I mean, once you fix those problems, then people don’t see them anymore.
Rovner: So let’s look forward quickly. It seemed at least for a while after the Republicans failed in 2017 to repeal and replace the law that efforts to undo it were finally over. But while this administration isn’t saying directly that they want to end it, they do have some big targets for undoing big pieces of it. What are some of those and what are the likelihood of them happening?
Levitt: Yeah, in some ways we have an ACA repeal-and-replace debate going on right now, just not in name. And there are really kind of two big pieces on the table. One, of course, is potential cuts to Medicaid. The House has passed a budget resolution calling for $880 billion in cuts, by the Energy and Commerce Committee, which has jurisdiction over Medicaid. The vast majority of those cuts would have to be in Medicaid. The math is simply inescapable. And a big target on the table is that expansion of Medicaid that was in the ACA.
And interestingly, you’re even hearing Republicans on the Hill talking about repealing the enhanced federal matching payments for the ACA Medicaid expansion and saying: Well, that’s not Medicaid cuts. That’s Obamacare. That’s not Medicaid. But 20 million people are covered under that Medicaid expansion. So it would lead to the biggest increase in the number of people uninsured we’ve ever had, if that gets repealed.
The other issue really has not gotten a lot of attention yet this year, which is the extra premium assistance that was passed under [President Joe] Biden and by Democrats in Congress. And that’s led to a dramatic increase in ACA marketplace enrollment. ACA enrollment has more than doubled to 24 million since 2020. Those subsidies expire at the end of this year. So if Congress does nothing, people would be faced with very big out-of-pocket premium increases. And I suspect it’s going to get more attention as we get closer to the end of the year, but so far there hasn’t been a big debate over it yet.
Rovner: Well, we’ll continue to talk about it. Larry Levitt, thank you so much.
Levitt: Oh, thanks. Great conversation.
Rovner: OK, we’re back. Now it’s time for our extra-credit segment. That’s where we each recognize the story we read this week we think you should read, too. Don’t worry if you miss it. We will put the links in our show notes on your phone or other mobile device. Joanne, why don’t you go first this week?
Kenen: There’s a piece in The Atlantic this week called “America Is Done Pretending About Meat,” by Yasmin Tayag, and it’s basically saying that half of the people who said they were vegan or vegetarian were lying and that meat is very much back in fashion. That the new pejorative term — some of us may remember from 20 years or so ago, the “quiche eaters” —now it’s the “soy boy.” And that one of the new “in” foods, and I think this is the first for the podcast to use the phrase, raw beef testicles. So when we’re talking about political red meat, it’s not just political red meat. America is, we’re eating a lot more meat than we said we did, and we’re no longer saying that we’re not eating it.
Rovner: Real red meat for the masses.
Ollstein: For what it’s worth, “soy boy” has been a slur since the Obama administration.
Kenen: Well, it’s just new to me. Thank you. I welcome the—
Ollstein: I unfortunately have been in the online fever swamps where people say things like that.
Kenen: Thank you, Alice. Now I know.
Rovner: Maya, why don’t you go next?
Goldman: My extra credit is a KFF Health News article by Rachana Pradhan and Aneri Pattani called “‘I Am Going Through Hell’: Job Loss, Mental Health, and the Fate of Federal Workers.” And I think it’s just worth remembering that there are real consequences, real mental health consequences to mass upheaval at the scale of what’s going on in the federal government right now with so many people losing their jobs and just not sure if their jobs are stable, especially in light of this morning’s news about HHS reorganizations. But also I think this article does a really good job of highlighting how this chaos and instability is only going to exacerbate already ongoing mental health crises that some of these workers that have been laid off were trying to help solve. And so it’s just this cycle that keeps running through. It’s worth remembering.
Rovner: The chaos is the point. Alice.
Ollstein: So, I have a piece from the New York Times Wirecutter section called “23andMe Just Filed for Bankruptcy. You Should Delete Your Data Now.” And it’s what it says. The company that millions and millions of people have sent samples of their DNA to over the years to find out what percent European they are and all this stuff and their propensity for various inherited diseases, that company is going bankrupt, and there is the expectation that it will be sold off for parts, including people’s very sensitive DNA. And the article points out that because they are not a health care provider, they are not subject to HIPAA [Health Insurance Portability and Accountability Act]. And so many elected officials and privacy advocates are recommending that people, very quickly, if they have given their DNA to this company, go and delete their information now before it gets sold off to who knows who.
Rovner: And for who knows what reason. My extra credit this week is something I really did think at first was from The Onion. It’s actually from CNN, and it’s called “State Lawmakers Are Looking to Ban Non-Existent ‘Chemtrails.’ It Could Have Real-Life Side Effects,” by Ramishah Maruf and Brandon Miller, who’s a CNN meteorologist. It seems that several states are moving to ban those white lines the jets leave behind them, on the theory that they are full of toxic chemicals and/or intended to manipulate the weather. In fact, they’re mostly just water vapor. They’re called contrails because the con is for condensation. But these laws could outlaw some new types of technologies that are aimed at addressing things like climate change. Clearly we need to teach more science along with more civics.
OK, that is this week’s show. As always, if you enjoy the podcast, you can subscribe wherever you get your podcast. We’d appreciate it if you left us a review. That helps other people find us, too. Thanks, as always, to our producer, Francis Ying, and our editor, Emmarie Huetteman. As always, you could email us your comments or questions. We’re at whatthehealth@kff.org. Or you can still find me at X, @jrovner, and at Bluesky, @julierovner. Where are you folks hanging these days? Maya?
Goldman: I am on X and Bluesky. If you search Maya Goldman, you’ll find me. And also increasingly on LinkedIn. Find me there.
Rovner: Hearing that a lot. Alice.
Ollstein: I am on X, @AliceOllstein, and Bluesky, @alicemiranda.
Rovner: Joanne.
Kenen: I’m mostly at Bluesky, and I’m also using LinkedIn a lot. @joannekenen at Bluesky. LinkedIn is reverberating more.
Rovner: All right, we’ll be back in your feed next week with still more breaking news. Until then, be healthy.
Credits
Francis Ying
Audio producer
Emmarie Huetteman
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
3 months 4 weeks ago
Courts, Health Industry, Multimedia, Public Health, States, Abortion, CDC, Georgia, HHS, KFF Health News' 'What The Health?', Misinformation, NIH, Podcasts, Pregnancy, reproductive health, texas, Trump Administration, U.S. Congress, vaccines, Women's Health

Harris apoya la reducción de la deuda médica. Los “conceptos” de Trump preocupan a defensores.
Defensores de pacientes y consumidores confían en que Kamala Harris acelere los esfuerzos federales para ayudar a las personas que luchan con deudas médicas, si gana en las elecciones presidenciales del próximo mes.
Y ven a la vicepresidenta y candidata demócrata como la mejor esperanza para preservar el acceso de los estadounidenses a seguros de salud. La cobertura integral que limita los costos directos de los pacientes es la mejor defensa contra el endeudamiento, dicen los expertos.
La administración Biden ha ampliado las protecciones financieras para los pacientes, incluyendo una propuesta histórica de la Oficina de Protección Financiera del Consumidor (CFPB) para eliminar la deuda médica de los informes de crédito de los consumidores.
En 2022, el presidente Joe Biden también firmó la Ley de Reducción de la Inflación, que limita cuánto deben pagar los afiliados de Medicare por medicamentos recetados, incluyendo un tope de $35 al mes para la insulina. Y en legislaturas de todo el país, demócratas y republicanos han trabajado juntos de manera discreta para promulgar leyes que frenen a los cobradores de deudas.
Sin embargo, defensores dicen que el gobierno federal podría hacer más para abordar un problema que afecta a 100 millones de estadounidenses, obligando a muchos a trabajar más, perder sus hogares y reducir el gasto en alimentos y otros artículos esenciales.
“Biden y Harris han hecho más para abordar la crisis de deuda médica en este país que cualquier otra administración”, dijo Mona Shah, directora senior de política y estrategia en Community Catalyst, una organización sin fines de lucro que ha liderado los esfuerzos nacionales para fortalecer las protecciones contra la deuda médica. “Pero hay más por hacer y debe ser una prioridad para el próximo Congreso y administración”.
Al mismo tiempo, los defensores de los pacientes temen que si el ex presidente Donald Trump gana un segundo mandato, debilitará las protecciones de los seguros permitiendo que los estados recorten sus programas de Medicaid o reduciendo la ayuda federal para que los estadounidenses compren cobertura médica. Eso pondría a millones de personas en mayor riesgo de endeudarse si enferman.
En su primer mandato, Trump y los republicanos del Congreso intentaron en 2017 derogar la Ley de Cuidado de Salud a Bajo Precio (ACA), un movimiento que, según analistas independientes, habría despojado de cobertura médica a millones de estadounidenses y habría aumentado los costos para las personas con afecciones preexistentes, como diabetes y cáncer.
Trump y sus aliados del Partido Republicano continúan atacando a ACA, y el ex presidente ha dicho que quiere revertir la Ley de Reducción de la Inflación, que también incluye ayuda para que los estadounidenses de bajos y medianos ingresos compren seguros de salud.
“Las personas enfrentarán una ola de deuda médica por pagar primas y precios de medicamentos recetados”, dijo Anthony Wright, director ejecutivo de Families USA, un grupo de consumidores que ha apoyado las protecciones federales de salud. “Los pacientes y el público deberían estar preocupados”.
La campaña de Trump no respondió a consultas sobre su agenda de salud. Y el ex presidente no suele hablar de atención médica o deuda médica en la campaña, aunque dijo en el debate del mes pasado que tenía “conceptos de un plan” para mejorar la ACA. Trump no ha ofrecido detalles.
Harris ha prometido repetidamente proteger ACA y renovar los subsidios ampliados para las primas mensuales del seguro creados por la Ley de Reducción de la Inflación. Esa ayuda está programada para expirar el próximo año.
La vicepresidenta también ha expresado su apoyo a un mayor gasto gubernamental para comprar y cancelar deudas médicas antiguas de los pacientes. En los últimos años, varios estados y ciudades han comprado deuda médica en nombre de sus residentes.
Estos esfuerzos han aliviado la deuda de cientos de miles de personas, aunque muchos defensores dicen que cancelar deudas antiguas es, en el mejor de los casos, una solución a corto plazo, ya que los pacientes seguirán acumulando facturas que no pueden pagar sin una acción más sustantiva.
“Es un bote con un agujero”, dijo Katie Berge, una cabildera de la Sociedad de Leucemia y Linfoma. Este grupo de pacientes fue una de más de 50 organizaciones que el año pasado enviaron cartas a la administración Biden instando a las agencias federales a tomar medidas más agresivas para proteger a los estadounidenses de la deuda médica.
“La deuda médica ya no es un problema de nicho”, dijo Kirsten Sloan, quien trabaja en política federal para la Red de Acción contra el Cáncer de la Sociedad Americana de Cáncer. “Es clave para el bienestar económico de millones de estadounidenses”.
La Oficina de Protección Financiera del Consumidor está desarrollando regulaciones que prohibirían que las facturas médicas aparezcan en los informes de crédito de los consumidores, lo que mejoraría los puntajes crediticios y facilitaría que millones de estadounidenses alquilen una vivienda, consigan un trabajo o consigan un préstamo para un automóvil.
Harris, quien ha calificado la deuda médica como “crítica para la salud financiera y el bienestar de millones de estadounidenses”, apoyó con entusiasmo la propuesta de regulación. “No se debería privar a nadie del acceso a oportunidades económicas simplemente porque experimentó una emergencia médica”, dijo en junio.
El compañero de fórmula de Harris, el gobernador de Minnesota, Tim Walz, quien ha dicho que su propia familia luchó con la deuda médica cuando era joven, firmó en junio una ley estatal que reprime el cobro de deudas.
Los funcionarios de la CFPB dijeron que las regulaciones se finalizarán a principios del próximo año. Trump no ha indicado si seguiría adelante con las protecciones contra la deuda médica. En su primer mandato, la CFPB hizo poco para abordarla, y los republicanos en el Congreso han criticado durante mucho tiempo a la agencia reguladora.
Si Harris gana, muchos grupos de consumidores quieren que la CFPB refuerce aún más las medidas, incluyendo una mayor supervisión de las tarjetas de crédito médicas y otros productos financieros que los hospitales y otros proveedores médicos han comenzado a ofrecer a los pacientes. Por estos préstamos, las personas están obligadas a pagar intereses adicionales sobre su deuda médica.
“Estamos viendo una variedad de nuevos productos financieros médicos”, dijo April Kuehnhoff, abogada senior del Centro Nacional de Derecho del Consumidor. “Estos pueden generar nuevas preocupaciones sobre las protecciones al consumidor, y es fundamental que la CFPB y otros reguladores supervisen a estas empresas”.
Algunos defensores quieren que otras agencias federales también se involucren.
Esto incluye al enorme Departamento de Salud y Servicios Humanos (HHS), que controla cientos de miles de millones de dólares a través de los programas de Medicare y Medicaid. Ese dinero otorga al gobierno federal una enorme influencia sobre los hospitales y otros proveedores médicos.
Hasta ahora, la administración Biden no ha utilizado esa influencia para abordar la deuda médica.
Pero en un posible anticipo de futuras acciones, los líderes estatales en Carolina del Norte recientemente obtuvieron la aprobación federal para una iniciativa de deuda médica que obligará a los hospitales a tomar medidas para aliviar las deudas de los pacientes a cambio de ayuda gubernamental. Harris elogió la iniciativa.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
9 months 1 week ago
Elections, Health Care Costs, Health Industry, Insurance, Noticias En Español, States, Biden Administration, Diagnosis: Debt, Investigation, Obamacare Plans, Trump Administration

Happening in Springfield: New Immigrants Offer Economic Promise, Health System Challenges
When Republican vice presidential candidate JD Vance claimed Haitian immigrants had caused infectious-disease rates to “skyrocket” in Springfield, Ohio, local health commissioner Chris Cook checked the records.
They showed that in 2023, for example, there were four active tuberculosis cases in Clark County, which includes Springfield, up from three in 2022. HIV cases had risen, but sexually transmitted illnesses overall were decreasing.
“I wouldn’t call it skyrocketing,” said Cook, noting that there were 190 active cases in 2023 in all of Ohio. “You hear the rhetoric. But as a whole, reportable infectious diseases to the health department are decreasing.”
Tensions are running high in this industrial town of about 58,000 people. Bomb threats closed schools and public buildings after GOP presidential nominee Donald Trump falsely claimed that Haitian immigrants — who he alleged were there illegally — were stealing and eating household pets. City and county officials disputed the claims the former president levied during his Sept. 10 debate with Vice President Kamala Harris, his Democratic opponent.
Trump was amplifying comments made by Vance that — along with his claims about the immigration status of this population — were broadly panned as false. When asked during a CNN interview about the debunked pet-eating rumor, Vance, a U.S. senator from Ohio, acknowledged that the image he created was based not on facts but on “firsthand accounts from my constituents.” He said he was willing “to create” stories to focus attention on how immigration can overrun communities.
But Ohio Gov. Mike DeWine, also a Republican, has said immigrants have been an economic boon to Springfield. Many began arriving because businesses in the town, which had seen its population decrease, needed labor.
Largely lost in the political rancor is the way Springfield and the surrounding area responded to the influx of Haitian immigrants. Local health institutions tried to address the needs of this new population, which had lacked basic public health care such as immunization and often didn’t understand the U.S. health system.
The town is a microcosm of how immigration is reshaping communities throughout the United States. In the Springfield area, Catholic charities, other philanthropies, volunteers, and county agencies have banded together over the past three to four years to tackle the challenge and connect immigrants who have critical health needs with providers and care.
For instance, a community health center added Haitian Creole interpreters. The county health department opened a refugee health testing clinic to provide immunizations and basic health screenings, operating on such a shoestring budget that it’s open only two days a week.
And a coalition of groups to aid the Haitian community was created about two years ago to identify and respond to immigrant community needs. The group meets once a month with about 55 or 60 participants. On Sept. 18, about a week after Trump ramped up the furor at the debate, a record 138 participants joined in.
“We have all learned the necessity of collaboration,” said Casey Rollins, director of Springfield’s St. Vincent de Paul, a nonprofit Catholic social services organization that has become a lifeline for many of the town’s Haitian immigrants. “There’s a lot of medical need. Many of the people have high blood pressure, or they frequently have diabetes.”
Several factors have led Haitians to leave their Caribbean country for the United States, including a devastating earthquake in 2010, political unrest after the 2021 assassination of Haiti’s president, and ongoing gang violence. Even when health facilities in the country are open, it can be too treacherous for Haitians to travel for treatment.
“The gangs typically leave us alone, but it’s not a guarantee,” said Paul Glover, who helps oversee the St. Vincent’s Center for children with disabilities in Haiti. “We had a 3,000-square-foot clinic. It was destroyed. So was the X-ray machine. People have been putting off health care.”
An estimated 12,000 to 15,000 Haitian immigrants live in Clark County, officials said. About 700,000 Haitian immigrants lived in the United States in 2022, according to U.S. Census data.
Those who have settled in the Springfield area are generally in the country legally under a federal program that lets noncitizens temporarily enter and stay in the United States under certain circumstances, such as for urgent humanitarian reasons, according to city officials.
The influx of immigrants created a learning curve for hospitals and primary care providers in Springfield, as well as for the newcomers themselves. In Haiti, people often go directly to a hospital to receive care for all sorts of maladies, and county officials and advocacy groups said many of the immigrants were unfamiliar with the U.S. system of seeing primary care doctors first or making appointments for treatment.
Many sought care at Rocking Horse Community Health Center, a nonprofit, federally qualified health center that provides mental health, primary, and preventive care to people regardless of their insurance status or ability to pay. Federally qualified health centers serve medically underserved areas and populations.
The center treated 410 patients from Haiti in 2022, up more than 250% from 115 in 2021, according to Nettie Carter-Smith, the center’s director of community relations. Because the patients required interpreters, visits often stretched twice as long.
Rocking Horse hired patient navigators fluent in Haitian Creole, one of the two official languages of Haiti. Its roving purple bus provides on-site health screenings, vaccinations, and management of chronic conditions. And this school year, it’s operating a $2 million health clinic at Springfield High.
Many Haitians in Springfield have reported threats since Trump and Vance made their town a focus of the campaign. Community organizations were unable to identify any immigrants willing to be interviewed for this story.
Hospitals have also felt the impact. Mercy Health’s Springfield Regional Medical Center also saw a rapid influx of patients, spokesperson Jennifer Robinson said, with high utilization of emergency, primary care, and women’s health services.
This year, hospitals also have seen several readmissions for newborns struggling to thrive as some new mothers have trouble breastfeeding or getting supplemental formula, county officials said. One reason: New Haitian immigrants must wait six to eight weeks to get into a program that provides supplemental food for low-income pregnant, breastfeeding, or non-breastfeeding postpartum women, as well as for children and infants.
At Kettering Health Springfield, Haitian immigrants come to the emergency department for nonemergency care. Nurses are working on two related projects, one focusing on cultural awareness for staff and another exploring ways to improve communication with Haitian immigrants during discharge and in scheduling follow-up appointments.
Many of the immigrants are able to get health insurance. Haitian entrants generally qualify for Medicaid, the state-federal program for the low-income and disabled. For hospitals, that means lower reimbursement rates than with traditional insurance.
During 2023, 60,494 people in Clark County were enrolled in Medicaid, about 25% of whom were Black, according to state data. That’s up from 50,112 in 2017, when 17% of the enrollees were Black. That increase coincides with the rise of the Haitian population.
In September, DeWine pledged $2.5 million to help health centers and the county health department meet the Haitian and broader community’s needs. The Republican governor has pushed back on the recent national focus on the town, saying the spread of false rumors has been hurtful for the community.
Ken Gordon, a spokesperson for the Ohio Department of Health, acknowledged the difficulties Springfield’s health systems have faced and said the department is monitoring to avert potential outbreaks of measles, whooping cough, and even polio.
People diagnosed with HIV in the county increased from 142 residents in 2018 to 178 to 2022, according to state health department data. Cook, the Clark County health commissioner, said the data lags by about 1.5 years.
But Cook said, “as a whole, all reportable infections to the health department are not increasing.” Last year, he said, no one died of tuberculosis. “But 42 people died of covid.”
Healthbeat is a nonprofit newsroom covering public health published by Civic News Company and KFF Health News. Sign up for its newsletters here.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
9 months 2 weeks ago
Elections, Health Industry, Public Health, Race and Health, States, Healthbeat, Immigrants, Ohio

Employers Haven’t a Clue How Their Drug Benefits Are Managed
Most employers have little idea what the pharmacy benefit managers they hire do with the money they exchange for the medications used by their employees, according to a KFF survey released Wednesday morning.
Most employers have little idea what the pharmacy benefit managers they hire do with the money they exchange for the medications used by their employees, according to a KFF survey released Wednesday morning.
In KFF’s latest employer health benefits survey, company officials were asked how much of the rebates collected from drugmakers by pharmacy benefit managers, or PBMs, is returned to them. In recent years, the pharmaceutical industry has tried to deflect criticism of high drug prices by saying much of that income is siphoned off by the PBMs, companies that manage patients’ drug benefits on behalf of employers and health plans.
PBM leaders say they save companies and patients billions of dollars annually by obtaining rebates from drugmakers that they pass along to employers. Drugmakers, meanwhile, say they raise their list prices so high in order to afford the rebates that PBMs demand in exchange for placing the drugs on formularies that make them available to patients.
Leaders of the three largest PBMs — CVS Caremark, Optum RX and Express Scripts — all testified in Congress in July that 95% to 98% of the rebates they collect from drugmakers flow to employers.
For KFF’s survey of 2,142 randomly selected companies, officials from those with 500 or more employees were asked how much of the rebates negotiated by PBMs returned to the company as savings. About 19% said they received most of the rebates, 27% said some, and 16% said little. Thirty-seven percent of the respondents didn’t know.
While a larger percentage of officials from the largest companies said they got most or some of the rebates, the answers — and their contrast with the testimony of PBM leaders — reflect the confusion or ignorance of employers about what their drug benefit managers do, said survey leader Gary Claxton, a senior vice president at KFF, a health information nonprofit that includes KFF Health News.
“I don’t think they can ever know all the ways the money moves around because there are so many layers, between the wholesalers and the pharmacies and the manufacturers,” he said.
Critics say big PBMs — which are parts of conglomerates that include pharmacies, providers, and insurers — may conceal the size of their rebates by conducting negotiations through corporate-controlled rebate aggregators, or group purchasers, mostly based overseas in tax havens, that siphon off a percentage of the cash before it goes on the PBMs’ books.
PBMs also make money by encouraging or requiring patients to use affiliated specialty pharmacies, by skimping on payments to other pharmacies, and by collecting extra cash from drug companies through the federal 340B drug pricing program, which is aimed at lowering drug costs for low-income patients, said Antonio Ciaccia, CEO of 46brooklyn Research.
The KFF survey indicates how little employers understand the PBMs and their pricing policies. “Employers are generally frustrated by the lack of transparency into all the prices out there,” Claxton said. “They can’t actually know what’s true.”
Billionaire Mark Cuban started a company to undercut the PBMs by selling pharmaceuticals with transparent pricing policies. He tells Fortune 500 executives he meets, “You’re getting ripped off, you’re losing money because it’s not your core competency to understand how your PBM and health insurance contracts work,” Cuban told KFF Health News in an interview Tuesday.
Ciaccia, who has conducted PBM investigations for several states, said employers are not equipped to understand the behavior of the PBMs and often are surprised at how unregulated the PBM business is.
“You’d assume that employers want to pay less, that they would want to pay more attention,” he said. “But what I’ve learned is they are often underequipped, underresourced, and oftentimes not understanding the severity of the lack of oversight and accountability.”
Employers may assume the PBMs are acting in their best interest, but they don’t have a legal obligation to do so.
Prices can be all over the map, even those charged by the same PBM, Ciaccia said. In a Medicaid study he recently conducted, a PBM was billing employers anywhere from $2,000 to $8,000 for a month’s worth of imatinib, a cancer drug that can be bought as a generic for as little as $30.
PBM contracts often guarantee discounts of certain percentage points for generics and brand-name drugs. But the contracts then contain five pages of exclusions, and “no employer will know what they mean,” Ciaccia said. “That person doesn’t have enough information to have an informed opinion.”
The KFF survey found that companies’ annual premiums for coverage of individual employees had increased from an average of $7,739 in 2021 to $8,951 this year, and $22,221 to $25,572 for families. Among employers’ greatest concerns was how to cover increasingly popular weight loss drugs that list at $2,000 a month or more.
Only 18% of respondents said their companies covered drugs such as Wegovy for weight loss. The largest group of employers offering such coverage — 28% — was those with 5,000 or more employees.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
9 months 2 weeks ago
Health Care Costs, Health Industry, Insurance, Pharmaceuticals, Drug Costs, Prescription Drugs

Calif. Ballot Measure Targets Drug Discount Program Spending
Californians in November will weigh in on a ballot initiative to increase scrutiny over the use of health-care dollars — particularly money from a federal drug discount program — meant to support patient care largely for low-income or indigent people.
Californians in November will weigh in on a ballot initiative to increase scrutiny over the use of health-care dollars — particularly money from a federal drug discount program — meant to support patient care largely for low-income or indigent people. The revenue is sometimes used to address housing instability and homelessness among vulnerable patient populations.
Voters are being asked whether California should increase accountability in the 340B drug discount program, which provides money for community clinics, safety net hospitals and other nonprofit health-care providers.
The program requires pharmaceutical companies to give drug discounts to these clinics and nonprofit entities, which can bank revenue by charging higher reimbursement rates.
Advocates pushing the measure, Proposition 34, say some entities are using the drug discount program as a slush fund, plowing money into housing and homelessness initiatives that don’t meet basic patient safety standards. Researchers and advocates have called for greater oversight.
“There are 340B entities that are misusing these public dollars,” said Nathan Click, a spokesperson for the pro-Proposition 34 campaign. “The whole point of this program is to use this money to get more low-income people health-care services.”
The initiative wouldn’t bar 340B providers from using health-care funds for housing or homelessness programs. Instead, it targets providers that spend more than $100 million on purposes other than direct patient care over 10 years. It would mandate that 98 percentof 340B revenues go to direct patient care. It also targets 340B providers with health insurer contracts and pharmacy licenses and those serving low-income Medicaid or Medicare patients that have been dinged with at least 500 high-severity housing violations for substandard or unsafe conditions.
That has placed a bull’s eye on the Los Angeles-based AIDS Healthcare Foundation, a nonprofit that provides direct patient care via clinics and pharmacies in California and other states, including Illinois, Texas and New York. It also owns housing for low-income and homeless people.
A Los Angeles Times investigation found that many residents of AIDS Healthcare Foundation properties are living in deplorable, unhealthy conditions.
Michael Weinstein, the foundation’s president, disputes those claims and argues that Proposition 34 proponents, including real estate interests, are going after him for another ballot initiative that seeks to implement rent control in more communities across California.
“It’s a revenge initiative,” Weinstein said, arguing that the deep-pocketed California Apartment Association is targeting his foundation — and its health and housing operations — because it has backed ballot measures pushing rent control across California. “This is a two-pronged attack against us to defeat rent control.”
Weinstein is locked in a feud with the apartment association, the chief sponsor of the initiative, which has contributed handsomely to pass Proposition 34. Opponents argue that the initiative is “a wolf in sheep’s clothing.”
Weinstein acknowledged to KFF Health News that his nonprofit uses money from 340B drug discounts to support its housing initiatives but argued they are helping treat and house some of the most vulnerable people, who would otherwise be homeless.
The apartment association declined several requests for comment. But Proposition 34 backers say they aren’t going after rent control — or Weinstein and his nonprofit.
Supporters argue that “rising health care costs are squeezing millions of Californians” and say that the initiative would “give California patients and taxpayers much needed relief, and lowers state drug costs, while saving California taxpayers billions.”
If the initiative passes and 340B providers do not spend 98 percent of the revenue on direct patient care, they could lose their license to practice health care and their nonprofit status.
This article is not available for syndication due to republishing restrictions. If you have questions about the availability of this or other content for republication, please contact NewsWeb@kff.org.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
9 months 2 weeks ago
california, Elections, Health Care Costs, Health Industry, Pharmaceuticals, States, Drug Costs, Health Brief
An Arm and a Leg: Don’t Get ‘Bullied’ Into Paying What You Don’t Owe
Caitlyn Mai thought she did everything right. She called ahead to make sure her insurer would cover her cochlear implant surgery. She thought everything went according to plan but she still got a bill for the full cost of the surgery: more than $139,000.
What Caitlyn did next is a reminder of why a beloved former guest once said you should “never pay the first bill.” This episode of “An Arm and a Leg” is an extended version of the July installment of the “Bill of the Month” series, created in partnership with NPR.
Dan Weissmann
Host and producer of "An Arm and a Leg." Previously, Dan was a staff reporter for Marketplace and Chicago's WBEZ. His work also appears on All Things Considered, Marketplace, the BBC, 99 Percent Invisible, and Reveal, from the Center for Investigative Reporting.
Credits
Emily Pisacreta
Producer
Claire Davenport
Producer
Adam Raymonda
Audio wizard
Ellen Weiss
Editor
click to open the transcript
Don’t Get ‘Bullied’ Into Paying What You Don’t Owe
Dan: Hey there —
One morning when she was in eighth grade, Caitlin Mai did what she always did when she woke up.
Caitlyn Mai: Music has always been a big part of my life. And so I immediately put in my headphones and started putting on music as I was about to get out of bed and get ready. And I noticed my earbud in my right ear wasn’t working.
Dan: It was obvious, because on this Beatles tune she’d cued up, Eleanor Rigby, the vocals are almost all on the right-hand side, and she couldn’t hear them.
Caitlyn: I was like, that’s kind of weird. So I switched the earbuds and it worked fine. But then it was, the other one wasn’t working in my right ear. And I was like, what?
Dan: Yeah, confusing. And then she tried getting out of bed.
Caitlyn: I was so dizzy. It was my first time experiencing vertigo, and it was so severe, I couldn’t walk across the room without getting severely motion sick.
Dan: With that vertigo, Caitlin could barely walk at all. She had no sense of balance — that actually relies on a mechanism inside our ears. Later, doctors found she had lost 87 percent of her hearing on the right side.
Caitlyn: They think I just had some sort of virus that settled in my ear, and it damaged my ear. But I went to bed completely healthy the night before. Woke up, couldn’t hear out of my ear.
Dan: She had to learn how to walk all over again.
Caitlyn: I have to rely on my eyes. My friends still find it hilarious if I close my eyes, I fall over.
Dan: That was eighth grade. Caitlyn made it through high school, in Tulsa where she grew up without a lot of accommodations.
Caitlyn: Cause in middle school, early high school, you don’t want to bring attention to your disability. At least I really didn’t want to at the time. I was super anxious about that.
Dan: Catilyn’s 27 now, she works as a legal assistant in Oklahoma City. Her husband’s a lawyer. And for the longest time, she couldn’t access a tool that helps restore hearing for lots of people: Cochlear implants — small devices that stimulate nerves inside the ear.
The FDA didn’t approve them for just one ear until a couple of years ago. Last year, Caitlin got her insurance to approve one for her. She had surgery in December to insert the implant. And in January, an audiologist attached an external component to switch on Caitlin’s right-side hearing.
Caitlyn: She said, okay, at some point, you’re gonna start hearing some beeps, just say yes when you can hear them. And my husband said my face just, out of nowhere, lit up, and I go, yes! It was streaming directly to my cochlear implant. And I definitely started tearing up.
Dan: Then, two weeks later, Caitlin got an alert from the hospital on her phone.
Caitlyn: And I open it up, and I immediately started having a panic attack.
Dan: It was a bill for a hundred and thirty-nine thousand dollars. The full amount for Caitlin’s surgery.
Which, given that Caitlyn had gotten her insurance company’s OK for the procedure in advance, was a pretty big surprise. NPR featured Caitlyn’s story recently for a series they do with our pals at KFF Health News.
NPR HOST: Time now for the latest installment in our bill of the month series, where we dissect and explain confusing or outrageous medical bills.
Dan: I interviewed Caitlyn for that story. And we’re bringing you an expanded version here because Caitlin’s situation — well, it was a good story. And it made me curious about a couple things.
It also reminded me of some good advice we’ve heard here before — and it reminded me of an important colleague and teacher. And the bottom line to Caitlyn’s story? Stand up for yourself. Don’t cave. Make the next call.
This is An Arm and a Leg — a show about why health care costs so freaking much, and what we can maybe do about it. I’m Dan Weissmann. I’m a reporter, and I like a challenge — so our job on this show is to take one of the most enraging, terrifying, depressing parts of American life, and bring you something entertaining, empowering, and useful.
To get her insurance company’s approval, Caitlyn had already spent a lot of time — and a lot of money — in the months before surgery. For instance …
Caitlyn: To prove to insurance that a hearing aid wouldn’t work had to be fitted for a hearing aid and then do a couple hours of testing to prove, yep, it doesn’t help.
Dan: There were reviews with audiologists, with her surgeon, and an MRI to make sure there wasn’t too much scar tissue for an implant to take.
Caitlyn: That took a long time to get scheduled, get insurance to approve, pay for, then get back for another appointment. I counted up at one point — it’s like around eight or ten appointments that I had before the final, okay, let’s schedule surgery.
Dan: And — you caught that, right? Where she mentioned she had to get her insurance to approve paying for the MRI? Every one of these preliminary steps cost money, and she had to wrangle with her insurance to get their OK.
But of course even with her insurance saying yes, there were still copays, and deductibles, and what’s called co-insurance — where you pay a percentage of any bill from a hospital.
Which meant Caitlyn was chipping away at what’s called her out-of-pocket maximum: The most she could be on the hook for in a given calendar year. The surgery got scheduled for December — the same calendar year as all those tests — and she checked to see what she might have to pay.
Caitlyn: I looked at my little portal for insurance, I’m showing what’s left on my out-of-pocket max for the year is around 2,000, give or take, 200 dollars.
Dan: She called the insurance company to confirm that estimate. And then she cranked up her due diligence.
Caitlyn: I called the hospital, and I asked for the names of the anesthesiologist, the radiologist. I asked for all of the details of who is possibly going to be on my case. And then I turned around and I called insurance and I said, I want to make sure all of these physicians are going to be in network on this date.
Dan: Caitlyn had done her homework. Probably more than a lot of us would have thought to do. I asked her: How’d you get so diligent? And first, like a lot of folks I’ve talked with, she said: Having a major health issue as a kid — losing her hearing — gave her an early heads-up to watch out.
Caitlyn: A little bit was, uh, experience of my mom dealing with insurance battles with me growing up. I remember her running into issues with that.
Can: And she’s got some experts in her life now. Her brother and her sister in law work in health care. One of her best friends is a healthcare lawyer and had some tips.
Caitlyn: But honestly, I think a lot of it is I have anxiety, and so I was just really paranoid.
Dan: The surgery went great. And a few weeks later, Caitlyn was in the audiologist’s office, getting that external component attached, and hearing on her right side for the first time in 15 years. Caitlyn says it all took some getting used to.
Caitlyn: I remember those, like, first few days especially, it wasn’t really like I was hearing full sounds. It was kind of just different pitches. I wasn’t hearing the words and everything, it was just the breakdown of the different pitches. And they also were just so much higher than they should be.
Dan: So interesting. Radiolab may have already done this story — [but] I’m just like, let’s find out what that’s about.
Caitlyn: I love Radiolab.
Dan: Me too! Anyway, two weeks after she starts getting used to her new hearing situation, Caitlyn gets that alert on her phone.
Caitlyn: And it tells me I have a new invoice. And I was like, oh, awesome! I’m not stressed at all, I did my due diligence. I know it’s gonna be expensive, but affordable.
Dan: Except, right: It’s a hundred and thirty-nine thousand dollars! Six figures. The full amount for her surgery. You might remember, Caitlyn said she had a panic attack. That was literal: Heart palpitations, hyperventilating.
It took her 20 or 30 minutes to get calm enough to start making calls. And she says her insurance told her they hadn’t paid because the hospital had neglected to send something important.
Caitlyn: The itemized bill. Which has all the codes and everything,
Dan: Caitlyn says she immediately asked the hospital, in writing to send her insurance the itemized bill, and she says sent a follow-up a week later. But her phone kept pinging with alerts about owing the hospital a hundred and thirty-nine thousand dollars.
Caitlyn: The app so conveniently told me that I could sign up for monthly payments of 11,000 dollars a month, which is just so absurd.
Dan: After two weeks, she asked her insurance: Do you have that itemized bill yet? They didn’t. So she called the hospital again.
Caitlyn: The girl I spoke with said she was putting in a request to have it faxed to my insurance and that would take two to three weeks. And I said, hold on, it takes you two to three weeks to fax a document?
Dan: Answer: Apparently yes? And Caitlyn says even three weeks later, her insurance company still hadn’t gotten that itemized bill the hospital promised to fax.
And all this time Caitlyn was still getting notices from the hospital billing department. And the latest one said, “past due.” She tried something new: So she called the hospital and demanded they send the itemized bill directly to her, immediately. Which they did.
Caitlyn: So I turned around and faxed it to my insurance.
Dan: Yeah but, this did not end things, not yet. Caitlyn says she got more notices labeled past due. She fought her way to a direct conversation with a supervisor.
Caitlyn: They kept saying,‘well, a supervisor’s not available right now.’ I said, No, you’re finding a supervisor. I don’t care if they’re cutting their lunch short. I’m talking to a supervisor right now. I don’t care if I sound like a Karen. It’s been a long, long year already.
Dan: Eventually, Caitlyn got a supervisor on the line and got the supervisor to get permission from a manager to stop sending her bills while the hospital waited for insurance to pay.
By this time, it was late March, almost two months after that first bill gave Caitlyn that panic attack. Also by this time, Caitlyn had sent her bill to the folks at NPR and KFF Health News for that Bill of the Month feature they do.
Caitlyn: I was like, I just need to vent. And so I submitted it just to vent it out. Never expecting anyone to reach out.
Dan: But they did. And on April 9th, Caitlyn got a call from a regional Patient Service Center manager.
Caitlyn: And she was super nice and tried to be really apologetic, but never actually accepting any blame. Or outright saying,‘we’re so sorry.’ Just said, ‘I’m sorry for your frustration, that sounds awful.’
Dan: She DID tell Caitlyn that the hospital had received payment from her insurance. And that Caitlyn could expect a final bill within a week. And that instead of a hundred thirty nine thousand, it was gonna be one thousand, nine hundred eighty-two dollars and twenty-five cents.
Caitlyn: I said,‘yep, that actually matches what my insurance said,’ and she said,‘oh, you know what was left on your out-of-pocket, most people don’t,’ and I said,‘I’m very well versed in every dollar sign at this point in this entire case.’
Dan: Caitlyn says she got that bill four days later and paid it immediately.
Caitlyn: And I saved the receipt of that, I have saved everything. It feels like it’s resolved, but there’s part of me that’s still waiting for the other shoe to drop
Dan: So, Caitlyn’s story brings up a LOT. Of course, I loved the way she kept fighting, and ultimately took control of the situation. And I hated how she got trapped between these two big entities and how much time and stress the whole thing cost her.
Because, you know, the hospital could’ve resolved this so quickly by just sending that itemized bill to Caitlyn’s insurance company.
Caitlyn: And the hospital did not do that. They just turned around and billed me. Which was a stupid idea, since the insurance company is more likely to have the money. Not the legal assistant in Oklahoma.
Dan: Caitlyn’s story raised a few questions, and brought back a lot of themes we’ve touched on before. We dug in also found some new tips, and some memories I want to share. That’s coming right up.
This episode of An Arm and a Leg is a co-production of Public Road Productions and KFF Health News, a nonprofit newsroom covering healthcare in America. Their senior contributing editor, Elisabeth Rosenthal, reported Caitlyn’s story for KFF and NPR. She wrote a book about U.S. healthcare. It’s called “An American Sickness,” and it was an inspiration for this show.
One question we ask sometimes on this show when we see a bill that’s so wildly ridiculous and unfair is: Can they freaking DO that?!? Like, is that even legal?
Like in this instance, can they just keep billing you while they’re apparently not even playing ball with your insurance? And: Do we have any legal weapons to fight back with?
We asked a bunch of legal experts, and they pretty much all said: Yes, they probably can do that, and no, we probably don’t have any easy legal weapons we can fight with. But then I talked with Berneta Haynes. She’s a senior attorney with the National Consumer Law Center.
And she had some practical thoughts that are super-worth sharing. She used to work for a nonprofit called Georgia Watch — that’s a state-level consumer protection group. They operated a hotline people could call for help.
Berneta Haynes: Consumers and patients would call us with all kinds of hospital billing issues and medical debt issues. And we’ve had these kinds of weird questions where really, there wasn’t a particular lever at the legal level to actually help them. But if they feel like they’re experiencing what could be considered potentially an unfair business practice, it is totally within their right to file a complaint within their state A. G.’s office.
Dan: The A.G. The state attorney general. Whoever’s doing you wrong, you can file a complaint.
Berneta: Whether or not there’s any real hook that your AG could use to hold them accountable is always a question that’s up in the air. But even just the act of filing a complaint is very likely to get that entity, that company, to behave correctly.
Dan: Basically, go up the chain. Whether to a government watchdog, or in the organization that’s bugging you. We’ve heard this before, but I loved the specifics that Berneta Haynes shared with me about her own experiences.
Berneta: I will tell you, one of the mechanisms my husband and I have had to utilize repeatedly, not in a hospital context, but in various other service contexts is to reach out or threaten to reach out to the CEO or president. And it gets results every time. It gets results every time!
Dan: Oh, and here’s the pro tip.
Berneta: My husband has repeatedly, when he’s had to do it, set up a LinkedIn premium account just to find the CEO and message them directly.
Dan: Ooh, that’s good!
Berneta: That has been the way we’ve gotten resolution on all kinds of issues related to insurance companies not wanting to do right by us. And so forth.
Dan: So that was fun. Now, I do want to talk a little bit about what Caitlyn did, and what allowed her to do it. Caitlyn figures she made at least a dozen phone calls. And she says she’s lucky — privileged — to have a job where she could do that. Here’s the first thing she says she did once she got over that panic attack when the bill arrived.
Caitlyn: I just went to my boss’s office and I said, I’m going to have to make some phone calls. There’s a problem with my hospital bill. She’s like, don’t worry about it. Do what you need to.
Dan: And she had people in her corner, like the friend who’s a healthcare lawyer. And legal advice wasn’t the big thing that friend gave Caitlyn.
Caitlyn: Most of the time I was just venting to her, and she was like,‘you need to keep pushing, like, keep going at them. Don’t let them win. Don’t roll over. Just keep pushing. They should be paying.’
Dan: And at that point, I told Caitlyn, she and her story were really reminding me of someone.
Dan: There’s a reporter named Marshall Allen. He worked for ProPublica for a long time. He wrote on healthcare, and he wrote on stuff like this. And eventually he wrote a book, giving advice to people. And the title of the book was, Never Pay the First Bill.
Caitlyn: Oh!
Dan: And I told Caitlyn, Marshall was on my mind at the time because when Caitlyn and I talked in May, Marshall had just died, like less than two weeks before. And he was young — 52. He had three kids.
Caitlyn: So sad.
Dan: Super, super, super sad.
Dan: And of course the title of Marshall’s book — Never Pay the First Bill — that’s exactly how Caitlyn played things. She wasn’t going to think about paying anything until she got her questions answered. And it is worth remembering.
When we were talking with legal experts, one thing a few of them said was: If you pay something that insurance was supposed to cover, and then insurance comes through, you’re supposed to get a refund. But who wants to chase that?
Yeah. Don’t pay that first bill until you’ve made sure this is money you really owe. So, this seems like a good time to memorialize Marshall Allen a little bit. He liked to compare the healthcare system to a schoolyard bully. Here’s what he told me when he was on this show in 2021 when his book had just come out.
Marshall Allen: What I think we need to do is stand up to the bully. We need to stop being afraid. We need to stop thinking someone else is going to stick up for us. And I wrote the book to equip and empower people to stand up to the bullies.
And I think it’s tremendously empowering, but it’s hard, and standing up to a bully takes incredible courage. It takes fortitude. It takes persistence. You might get beat up in the process. There’s no guarantee of victory. It’s risky, right? But if we don’t try, we don’t have a chance.
Dan: Marshall was a Christian minister before he became a reporter. He wrote a thoughtful essay about how his work as an investigative reporter fit with his faith. The gist was: The Bible is pretty clear that cheating people and exploiting them is wrong.
And to me, it seems like there was an element of ministry– not just evangelism — to what he did after his book came out. Here’s what he told me in 2021:
Marshall: I’ve started taking calls, and I’m responding to emails that I get from people and I’m saying,‘call me, let’s talk it through, let me help you with this. Let’s work through this together.’ And now I’m helping people work through their bills, work through these situations where they’re being cheated. It’s super satisfying and gratifying, so it’s my new hobby.
Dan: He kept at it. He left ProPublica and took a job with the Office of the Inspector General at the federal department of Health and Human Services. And he published a newsletter — it was free, but he encouraged people to pay if they could, and he used the money to hire medical-bill advocates to help people with especially tricky cases.
And Marshall was funny. I want to close out this episode with a story he told me the first time we talked, in 2019. It’s kind of an origin story.
Marshall: So when I was 16 years old, um, I worked for this dinner theater in Golden, Colorado, where I grew up. One day I show up for work, and they’ve closed down the business. They owed me like three weeks of pay.
The guy had closed the place without paying us and said,‘there’s no money. We shut down the business. We can’t afford to pay you. You’re out of luck.’ Well, we were all pretty angry about that. We were really angry because they had opened a sister dinner theater under the same company umbrella across town. And we all knew that. And we were like, well, if you can afford to keep your other place open, you can afford to pay us. And they said,‘sorry, kids, you’re out of luck.’
Dan: Marshall goes home, tells his mom what’s going on.
Marshall: And my mom tells me you should sue him. I’m like, mom, what do you mean? I can barely drive. How can I sue the guy? She goes,‘you should take him to small claims court.’ So lo and behold, I go down, I fill out the paperwork.
It’s a few paragraphs. It’s easy to fill out the paperwork in small claims court. I fill out the paperwork and turn in like 10 bucks at the time or whatever it costs. It’s not that expensive to file one of these cases. And I get a notice in the mail like six weeks later. And I have a court date, and I’m like geared up for this big Perry Mason moment.
Dan: Perry Mason was a lawyer on this super old TV show — courtroom drama. But this wasn’t a courtroom.
Marshall: It’s more like a conference room and there’s some administrative hearing judge in there. And lo and behold, the owner of the company and his attorney had to show up in court there with me.
And I thought we’d have a big argument all the administrative judge did is he read my few paragraphs on the little thing I’d written up and he looks over at the owner and he goes,‘is what this kid saying true?’And the owner’s like, ‘well, yeah.’ And the judge is like,‘give this kid his money.’ And I was like, This is amazing. You know what? Maybe the court system does actually work every now and then maybe every now and then the little guy can win.
Dan: Marshall and I both stayed interested in how people can use the legal system to get our rights. I learned a lot from Marshall, and like a lot of people, I just loved his spirit. Marshall Allen, thank you. And here’s the end of my conversation with Caitlyn.
Dan: Marshall Allen would have been extremely proud of you.
Caitlyn: Yeah.
Dan: Caitlyn has the final word here.
Caitlyn: I got to the point where I was like, it’s my fight. I’ve got gasoline in the fire. I’m, I’m going for it.
Dan: We’ll be back with a new episode in a few weeks. Till then, take care of yourself.
This episode of An Arm and a Leg was produced by me, Dan Weissmann, with help from Emily Pisacreta and Claire Davenport — and edited by Ellen Weiss.
KFF senior contributing editor Elisabeth Rosenthal reported Caitlyn’s story for KFF and NPR. She was editor in chief there when she invited me to collaborate with KFF to make this show’s second season, and we’ve been colleagues ever since. I’ve never felt so lucky or so thankful.
Special thanks to Christopher Robertson at Boston University’s School of Law, Wendy Epstein of the College of Law at DePaul University, Sabrina Corlette at Georgetown University’s Center on Health Insurance Reforms, and Elisabeth Benjamin from the Community Service Society of New York for pitching in with legal expertise here.
Adam Raymonda is our audio wizard. Our music is by Dave Weiner and Blue Dot Sessions. Gabrielle Healy is our managing editor for audience. Bea Bosco is our consulting director of operations. Sarah Ballama is our operations manager.
An Arm and a Leg is produced in partnership with KFF Health News. That’s a national newsroom producing in-depth journalism about healthcare in America and a core program at KFF, an independent source of health policy research, polling, and journalism.
Zach Dyer is senior audio producer at KFF Health News. He’s editorial liaison to this show. And thanks to the Institute for Nonprofit News for serving as our fiscal sponsor. They allow us to accept tax-exempt donations. You can learn more about INN at INN.org. Finally, thank you to everybody who supports this show financially. You can join in any time at https://armandalegshow.com/support/. Thank you so much for pitching in if you can — and, thanks for listening.
“An Arm and a Leg” is a co-production of KFF Health News and Public Road Productions.
To keep in touch with “An Arm and a Leg,” subscribe to its newsletters. You can also follow the show on Facebook and the social platform X. And if you’ve got stories to tell about the health care system, the producers would love to hear from you.
To hear all KFF Health News podcasts, click here.
And subscribe to “An Arm and a Leg” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
11 months 23 hours ago
Health Care Costs, Health Industry, Insurance, Multimedia, An Arm and a Leg, Oklahoma, Out-Of-Pocket Costs, Podcasts, Surprise Bills

Readers Weigh In on Abortion and Ways To Tackle the Opioid Crisis
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
Debunking Abortion Myths
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
Debunking Abortion Myths
I want to send a big THANK YOU to Matt Volz for writing a fact-checking article on the nonsense rhetoric around “abortion up until and after birth” that has run wild and unchallenged in the media (“GOP’s Tim Sheehy Revives Discredited Abortion Claims in Pivotal Senate Race,” July 9). Thanks for putting abortion later in pregnancy in context and debunking false assumptions.
I am a near-third-trimester abortion patient (nonviable pregnancy, terminated at 26 weeks), and I am so sick of hearing politicians like Tim Sheehy talk about something they have never experienced or bothered to learn about. It is as though I am watching the entire nation maliciously gossip about me and other parents like me. Those of us in the termination for medical reasons (TFMR) community have walked through hell only to have our voices, at best, be ignored or, more commonly, be insulted and threatened.
And I imagine watching this political circus is just as hurtful for parents who lost an infant shortly after birth and had to provide palliative care. That is who they are talking about with “abortion after birth”; they are talking about comfort care for infants who will not survive.
Thank you again for bringing a dose of reality to a conversation that never should have become political. These are impossible decisions that only parents should make. It was really refreshing to read Volz’s article and know that some journalists are still willing to fact-check the absurd claims floating around. It was encouraging to know that someone does see us.
— Anne Angus, Bozeman, Montana
A physician and Yale professor of radiology and biomedical imaging took to the social platform X to share feedback:
.@SenatorTester is a great Senator. And his opponent is a great liar. Both the GOP presidential candidate and Tim Sheehy have perpetuated this lie. Please push back every time you hear it. https://t.co/1LBGPgOA2u
— (((Howard Forman))) (@thehowie) July 9, 2024
— Howard Forman, New Haven, Connecticut
I just read your article at PolitiFact on Republican Senate candidate Tim Sheehy’s statement about abortion, and I would like to point out (what I believe) are a couple of errors.
1. In paragraph 10, you quote KFF’s Alina Salganicoff saying that “in the good-faith medical judgment of the treating health care provider, continuation of the pregnancy would pose a risk to the pregnant patient’s life or health.” Now, you may know that almost at the same time that the Roe v. Wade decision was released, there was a decision called Doe v. Bolton that interpreted “health” to mean almost anything. That broad interpretation of health is found in your article in paragraph 24: “Women have abortions later in pregnancy either because they find out new information or because of economic or political barriers,” [Katrina] Kimport said.
When a woman can have an abortion after viability because she offers any reason that can be interpreted as “health,” then abortion would be legal throughout all nine months of pregnancy. I believe that you are wrong in your interpretation. Democrats do not want to name any restriction on abortion during all nine months, and every mention of “health” is a fig leaf that does not restrict abortion at all. Every abortion advocate knows that.
2. Whether late-term abortions are rare or not is logically irrelevant to whether late-term abortions should be restricted.
Why don’t you know these things?
— Darryl A. Linde, Tahlequah, Oklahoma
An Air Force veteran added his two cents on X:
Dems have the facts. Republicans spread fear and lies.https://t.co/6CWfKhqxJZ
— James Knight (@jamesUSAF_vet) July 12, 2024
— James Knight, Reno, Nevada
Making a Healthy Difference for the Homeless
Thank you for printing this story (“A California Medical Group Treats Only Homeless Patients — And Makes Money Doing It,” July 19). It really piqued my interest and portrayed a positive solution for getting care to the people.
Up here in the Bay Area, I believe there are a couple of groups who go out and find what needs doing instead of waiting for people to come to them — but nothing like this. Makes me curious about what we actually have going on here.
— Laurie Lippe, El Cerrito, California
A self-described “nurse turned health tech nerd” commended the effort on X:
"They distribute GPS devices so they can track their homeless patients. They keep company credit cards on hand in case a patient needs emergency food or water, or an Uber ride to the doctor"This is healthcare at its best 💕https://t.co/UhM1dgTPH7
— Rik Renard (@rikrenard) July 22, 2024
— Rik Renard, New York City
A senior policy director at the National Health Care for the Homeless Council shared the post on X — while stressing that her tweets reflected her own opinions and not those of her organization:
I’m with @DrJimWithers: “I do worry about the corporatization of street medicine and capitalism invading what we’ve been building, largely as a social justice mission outside of the traditional health care system.” https://t.co/IOjazvrvqP
— Barbara DiPietro (@BarbaraDiPietro) July 19, 2024
— Barbara DiPietro, Baltimore
On X, a physician who says she champions “physicians, patients, public health, and the patient-physician relationship” reacted to our coverage surrounding the Federal Trade Commission’s rule banning the use of noncompete agreements in employment contracts:
FTC #noncompete crackdown may not protect doctors and nurses at ~64% of US community hospitals that are tax-exempt nonprofits or government-owned.But, @FTC said some nonprofits could be bound by the rule if they do not operate as true charities. https://t.co/9fDbfVflTH
— Marilyn Heine (@MarilynHeineMD) May 28, 2024
— Marilyn Heine, Langhorne, Pennsylvania
Without a Noncompete Ban on All Employers, Rural Access to Care Suffers
When news broke that the Federal Trade Commission would be banning noncompete agreements in employment contracts, many of us in the medical profession celebrated. However, until nonprofit hospitals and health care facilities benefit from the same ban, access to care — particularly in rural regions — will suffer.
As reported in “Health Worker for a Nonprofit? The New Ban on Noncompete Contracts May Not Help You” (June 5), about two-thirds of U.S. community hospitals are nonprofit or government-owned. This means that most hospitals nationwide may continue to enforce noncompete agreements among their employees, a practice that will have an outsize impact on rural medical professionals.
As a rheumatologist in a rural area, I’ve seen how detrimental limited access to care is for patients. Noncompete agreements serve only to further limit access to much-needed care. Due to the physician shortage being particularly acute in rural America, there are oftentimes only a few specialty physicians servicing a large region. Suppose one of these specialists is employed by a large health system and wants to transition to a private practice. It reduces the number of accessible specialists in the area when their noncompete agreement prohibits them from practicing near any of the health care facilities associated with the system. And increasing consolidation across health care means many rural regions may have only a single health system that operates across the entire state and surrounding areas. A geographically limiting noncompete agreement essentially stops a physician or medical professional from practicing entirely in the area, or they must uproot their life and move away from the major health system.
I hope the FTC takes further action to include nonprofit health care employers in its noncompete ban. I also urge nonprofit employers to consider their rural patients’ access to care when requiring providers to sign noncompete agreements. It’s in the best interest of our patient’s health to get rid of these agreements entirely.
— Chris Phillips, chair of the American College of Rheumatology’s Committee on Rheumatologic Care, Paducah, Kentucky
The president of the Texas Medical Board also posted on X with feedback:
Is it a coincidence that this affects everyone, except those who work for nonprofit hospitals and health care facilities, which employs the largest number of medical professionals?The FTC and it's selective enforcement and rules is blatantly obvious! https://t.co/RzXInqiJ8D
— Sherif Zaafran, MD (@szaafran) June 16, 2024
— Sherif Zaafran, Houston
Repurposing Newspaper Boxes for Public Health
I recently read your article by Mara Silvers regarding the state’s intended use of public health vending machines (PHVMs) to help fight the opioid overdose epidemic (“Montana’s Plan To Curb Opioid Overdoses Includes Vending Machines,” July 18). Working on the covid-19 response for almost four years now, and with our American Rescue Plan Act funding coming to an end, we recently used a byline in our equipment budget to purchase and place “resource kiosks” in the community.
In 2022, after researching the use of vending machines for test distribution, we discovered vending machines have high barrier-to-entry costs and high maintenance costs. And even if purchasing isn’t possible, rental contracts come with high fees. We decided it was better to use a lower-cost resource that could be purchased in greater quantity, easily placed with community partners, and required no maintenance: the refurbished newspaper kiosk.
We decided to purchase double-decker boxes, which have a secondary door, creating another shelf, for roughly $410 apiece and stocked them with covid tests, nasal naloxone, injectable naloxone, fentanyl test strips, xylazine test strips, various types of condoms, and lubrication packets. We are in the process of securing a supply of gun locks and adding links to our pilot landing page for individual free gun lock deliveries, as well as links for free sexually transmitted infection test kits. We have investigated providing dental supplies and other items, but long-term funding is a constant concern. Grant money for most programs (likely all ARPA dollars) is running out, so the viability of these types of pilot programs is tentative without a buy-in from state or federal agencies.
Mara’s article hinted at criteria for possible placements and, similarly, we didn’t use locational overdose data, which can be “othering” to communities, but instead placed these kiosks with community partners that have been accomplished supporters of their at-risk populations throughout the covid response. Each community partner helped protect the communities they served through increased access to resources and provided information as trusted messengers. Truly meeting people where they are.
While money quickly appeared to fight the covid pandemic, and states spirited away dollars for pet projects, that sea of funding has dried up, and there doesn’t seem to be a plan for any continued funding. Covid-related functions have all been folded back into communicable disease epidemiology programs, which were already underfunded; in our state, the money funding the naloxone bulk fund is also drying up. Covid deaths might be down, but there is always a new bug (H5N1), STI infections are up, and gun-related deaths grow year over year. Funding population-level health interventions is our next pandemic.
With enough funding, kiosk-sized PHVMs could be swiftly added to any public health agency’s or community program’s quiver of tools to help increase access to resources and information for the most vulnerable residents.
Thank you for publishing a great article about the emerging opportunities to respond to changing public health needs!
— Christopher Howk, Arapahoe County Public Health’s covid-19 testing and logistics coordinator, Greenwood Village, Colorado
A retiree with a PhD in quantum chemistry tweeted his surprise over the news:
Montana’s Plan To Curb Opioid Overdoses Includes Vending Machineshttps://t.co/kNxYjnIOEO(What???!! Vending machines for opioids?)
— John Lounsbury (@jlounsbury59) July 18, 2024
— John Lounsbury, Lake Frederick, Virginia
Misappropriation of Opioid Settlement Funds
OK, so I see how all these states got all these lump sums of money for people like us who became addicted and whose lives were devastated by Purdue Pharma, Vicodin, and all the pharmacies (“Lifesaving Drugs and Police Projects Mark First Use of Opioid Settlement Cash in California,” July 12). How come all these states got all the money but those of us who have suffered have to wait, hire lawyers, and wait years for the money that was just handed over to these states? We’re the ones whose lives were devastated. My son was hooked, I was hooked, and my wife, and yet we must sit here penniless after the addiction, while all these states take the money — and they don’t do what they’re supposed to with it, and everyone knows it.
— Michael Stewart, Des Moines, Iowa
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
11 months 4 weeks ago
Health Industry, Public Health, Rural Health, Abortion, Homeless, Letter To The Editor, Misinformation, Opioids, Substance Misuse, Women's Health