Puerto Rico has declared an epidemic following a sharp rise in dengue cases - PBS NewsHour
- Puerto Rico has declared an epidemic following a sharp rise in dengue cases PBS NewsHour
- Puerto Rico declares dengue a public health emergency University of Minnesota Twin Cities
- Dengue fever alert: Puerto Rico declares epidemic USA TODAY
- Puerto Rico declares public health emergency after spike in dengue cases Healio
- Puerto Rico Declares Health Emergency Over Dengue MSN
1 year 7 months ago

Merck’s next big thing is (probably) on the way
1 year 7 months ago
Biotech, Business, Health, Pharma, Politics, The Readout, Biotech, biotechnology, drug development, drug prices, drug pricing, finance, genetics, government agencies, Pharmaceuticals, Research
CEMDOE presents innovative nursing training program
1 year 7 months ago
Health, CEMDOE, diabetes, nursing personnel, Obesity, Specialties Medical Center
Health Archives - Barbados Today
Nurses urge speeded-up compact talks
1 year 7 months ago
Health, Local News
Hospitals make leadership appointments
1 year 7 months ago
News, appointments, Damien O’Dowd, Prof Anne-Marie Brady, Saint John of God Hospital, Tallaght University Hospital

Medical News, Health News Latest, Medical News Today - Medical Dialogues |
Bharat Biotech begins clinical trial of Tuberculosis vaccine MTBVAC in India
1 year 7 months ago
News,Industry,Pharma News,Latest Industry News
Puerto Rico declares epidemic after spike in dengue cases - The Associated Press
- Puerto Rico declares epidemic after spike in dengue cases The Associated Press
- Puerto Rico has declared an epidemic following a sharp rise in dengue cases PBS NewsHour
- Dengue fever alert: Puerto Rico declares epidemic USA TODAY
- Puerto Rico's Mosquitoes Continue Carrying Dengue and Zika Viruses Precision Vaccinations
- Pandemic threat disease grips US as mosquito-borne virus attacks Puerto Rico MSN
1 year 7 months ago

AbbVie Gets Another Ulcerative Colitis Contender via $137M Landos Acquisition
1 year 7 months ago
BioPharma, Pharma, Top Story, AbbVie, biopharma nl, Clinical Trials, immunology, inflammation, inflammatory bowel disease, Landos Biopharma, ulcerative colitis, Virinia
Covid-19 After Action Review can result in improvement
1 year 7 months ago
Health, cerc, contingent emergency response component, coronavirus, COVID-19, linda straker, phillip telesford, shawn charles, world bank
Health – Demerara Waves Online News- Guyana
Guyana govt approves private sector recruitment of foreign health-care workers; not limited to Bangladeshis- Todd
1 year 7 months ago
Business, Health, News, Politics
Medical News, Health News Latest, Medical News Today - Medical Dialogues |
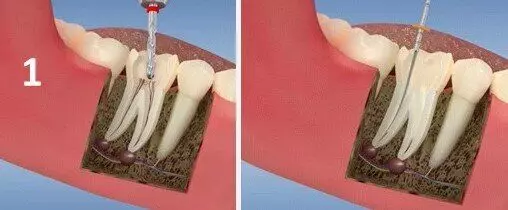
Vital pulp therapy tied to less postoperative pain compared to single visit root canal treatment: Study
1 year 7 months ago
Dentistry News and Guidelines,Top Medical News,Dentistry News
Health Archives - Barbados Today
Fogging schedule for March 25 – 28
1 year 7 months ago
Health, Local News
T&T health minister urges PANCAP to help Caribbean cure HIV
1 year 7 months ago
News, managers, NAPS, PANCAP, T&T health Minister, Terrence Dyalsingh
Medical News, Health News Latest, Medical News Today - Medical Dialogues |
Health Bulletin 23/ March/ 2024
1 year 7 months ago
MDTV,Channels - Medical Dialogues,Health News today MDTV,Health News Today

Medical News, Health News Latest, Medical News Today - Medical Dialogues |
USFDA grants full approval for Abbvie Elahere for certain ovarian cancer patients
1 year 7 months ago
News,Obstetrics and Gynaecology,Oncology,Obstetrics and Gynaecology News,Oncology News,Industry,Pharma News,Latest Industry News