Infectious disease doctor says COVID testing is vital this fall as symptoms are less severe or obvious - CBS News
- Infectious disease doctor says COVID testing is vital this fall as symptoms are less severe or obvious CBS News
- Can you get COVID-19 and the flu at the same time? A Mayo Clinic expert weighs in Mayo Clinic
- Fall vaccines: What to know about flu, COVID-19 and RSV shots Daily Herald
- Pharmacy sees interest for flu, COVID and RSV vaccines headed into winter months KCRG-TV9: Your Trusted Local News Source
- WHMI 93.5 Local News : CDC Forecasts Severity of 2023-24 Flu Season WHMI
- View Full Coverage on Google News
2 years 3 weeks ago
Father of girl who died of dengue fever requests state of emergency from the president
Amid grief for the loss of his 13-year-old daughter, urologist José Ezequiel Pérez Durán called on the authorities to take measures against the outbreak of dengue fever that continues to wreak havoc on the Dominican child population.
Perez Duran asked President Abinader to pay attention to the growing 0epidemic, about which he indicated the figures do not correspond to reality, so he asked to declare a state of emergency in the country due to increased cases.
“I am making a call to you, Mr. President (…), I understand that within 24 hours you should decree a state of emergency, where a campaign of fumigation, orientation, protocolization of the dengue fever that we have in front of us,” said the doctor.
The doctor’s daughter died on Friday last week after remaining in intensive care and being diagnosed with the disease transmitted by the Aedes Aegypti mosquito after being hospitalized since Wednesday morning.
He explained that the teenager arrived at the hospital “in a critical condition,” so she was immediately referred to the Intensive Care Unit.
“We as parents spared neither resources nor efforts to facilitate everything that was asked of us,” said the grieving father in an interview with Martina Espinal on the program Al Punto.
He indicated that, at first, they thought it was a classic dengue, but after she was intubated early Thursday morning, the infant became brain-dead at 5:00 p.m., indicating to her parents that it was too late.
The girl’s father said that the child’s platelets, which were at 266, reached 11 in just three days.
With a troubled expression, Perez narrated that they took the girl to receive medical attention since the first symptoms appeared on Sunday of that week. However, the pre-adolescent died days later.
“On Friday morning an attempt was made to connect her to a special dialysis machine, when the caveat was made that the girl was clinically dead, it was literally exploding her lungs, heart and kidneys. When she was connected to the machine, the girl died after two minutes, she went into irreversible arrest,” he said.
2 years 3 weeks ago
Health, Local
Breast cancer hope | Lead Stories - Jamaica Gleaner
- Breast cancer hope | Lead Stories Jamaica Gleaner
- How close are we to a cure for metastatic breast cancer? Labiotech.eu
- View Full Coverage on Google News
2 years 3 weeks ago
Breast cancer hope | Lead Stories - Jamaica Gleaner
Breast cancer hope | Lead Stories
Jamaica Gleaner
2 years 3 weeks ago
Cancer in children is different from cancer in adults - Jamaica Gleaner
- Cancer in children is different from cancer in adults Jamaica Gleaner
- Kids coping with cancer | Opinion | postandcourier.com Charleston Post Courier
- View Full Coverage on Google News
2 years 3 weeks ago
Food safety: Who is responsible in Jamaica?
EVERYONE on the food safety value chain is responsible for ensuring that food is handled and prepared safely.
Consequentially, the Government, farmers and other producers, food transporters, food business operators, food handlers, and customers are all responsible for ensuring a safe food supply nationally.
EVERYONE on the food safety value chain is responsible for ensuring that food is handled and prepared safely.
Consequentially, the Government, farmers and other producers, food transporters, food business operators, food handlers, and customers are all responsible for ensuring a safe food supply nationally.
Responsibilities of the Jamaican Government
Presently in Jamaica there are multi-government agencies with overlapping responsibilities for regulating food safety. The Government of Jamaica therefore needs to establish a regulatory mandate that clearly outlines the roles and responsibilities of each agency. This mandate is needed so that regulatory agencies can be more efficient in carrying out their functions.
A new approach to food handlers' certification in Jamaica is also necessary at this time; this new approach will allow for greater accountability and vigilance at all levels of the food supply value chain. For too long has the food handling industry operated without mandatory requirements, such as the employment of persons trained at the level of a food safety manager within food establishments.
This requirement is particularly important based on the size and nature of the operation. Food safety managers are individuals trained at an advanced level in food safety. According to international best practices, high-risk food establishments employing more than five persons are required by law in many countries to employ a food safety manager. Food safety managers are employed by food industry operators to ensure the implementation of regulatory requirements, enforcement of food safety standards and policies, as well as the evaluation of food handling practices, in order to gain compliance with legal guidelines within the food premises.
As of 2019 it is estimated that worldwide there are 9 million cases of typhoid fever occurring annually, resulting in about 110,000 deaths per year. Whilst the risk of typhoid fever is low in Jamaica, it cannot be forgotten that there have been numerous incidences of the disease reported amongst the local population — and even when symptoms no longer exist, approximately 5 per cent of the reported cases will be chronic carriers. Chronic carriers of typhoid have the potential to make others sick, especially through food and in situations where there is poor personal hygiene and sanitation practices.
A more stringent and comprehensive food handlers' certification system is therefore required, not just to ensure that the nation advances towards having individuals who are trained at a higher level in food safety but also for the institution of a system that will prevent those persons who are carriers of infectious food-borne diseases from being certified as fit for handling food.
Shared responsibility between government, food manufacturers, food processors
To date in Jamaica there is no mandatory or regulatory requirement for food processors and manufacturers to implement a food safety management system within their establishment; yet food recalls, food allergen management issues, the absence of systems to ensure the prevention of food-borne illness, and other related food safety issues are amongst the many problems associated with food manufacturing and processing. Mandatory implementation of appropriate processes and technologies throughout the supply chain, such as in food production facilities, is the most efficient method to guarantee that customers receive food that complies with the essential food safety standards. The implementation of food safety management systems such as Hazard Analysis Cortical Control Point (HACCP), Safe Quality Foods (SQF), and International Standards Organization 2200 (ISO 2200) should not be discretionary and done mostly in food production facilities exporting their goods. Agreeably, the implementation of such systems is not for everyone in the industry, however the health of the population needs to be protected by the implementation of proactive systems of food safety management that identify hazards ahead of time so as to avert any associated risk.
Urbanisation as well as some economic factors have led to more persons demanding cheaper food on the go in Jamaica. Street food vending provides such an option for the Jamaican populace. Street food vending is also enshrined in the culture of many countries including Jamaica, albeit the food safety risks associated with street food operations are no less than those that operate within fixed food establishments. Improper food handling practices, poor hand hygiene practices, improper solid waste management, absence of potable running water, inadequate food protection, failure to observe required temperatures for food, and lack of access to toilet facilities have always been some of the many environmental health challenges associated with these types of operations. The need to regulate the industry and license those establishments which are licensable should no longer be disregarded.
Shared responsibility between government and consumers
Like all other stakeholders in the food safety value chain, consumers have a role to play in ensuring that food safety standards are maintained on the food safety value chain. The time has therefore come for Jamaican consumers to educate themselves about food safety requirements; consumers should also become more vocal on non-compliance issues. In support to the responsibilities of the consumer is the need for the institution of a regulated food establishment rating system nationally. A system that supports publicly displayed scores and ratings of food establishments will encourage food business operators' compliance with regulatory requirements while at the same time allow the consumer to make informed choices prior to conducting business with a food establishment.
Shared responsibility between government regulatory agencies and food establishment operators
Surveillance data must guide the operations of a food regulatory system; the Government is therefore responsible for providing laboratory services for testing of food and safeguarding against all associated food safety hazards. Surveillance systems that capture incidence of food-borne illnesses and associated symptoms will also provide valuable information for timely public health response.
All food manufacturers and distributors, as well as others on the food safety continuum, should be required to implement traceability systems. It is therefore imperative that food safety regulators across ministries collaborate and promulgate a national food recall policy for the food industry. A national food recall policy will allow for the rapid identification and withdrawal of unsafe food lots in a timely manner — thereby averting public health catastrophes.
Dr Karlene Atkinson is a public health specialist and lecturer at the School of Public Health, University of Technology, Jamaica.
2 years 3 weeks ago
JN Group providing 150 free mammograms for Breast Cancer Awareness Month
FOR the sixth renewal of its Power of Pink breast cancer awareness campaign, JN Group will be financing 150 mammograms for women. The free screenings will be made available on World Mammography Day, October 20.
Saniah Spencer, marketing executive at JN Group, says the initiative has been made possible through a collaboration with member company, JN Money Services, and the Jamaica Cancer Society (JCS). The services will be offered through the JCS at its headquarters on Lady Musgrave Road in St Andrew.
"Mammograms are costly for several women and are not as readily accessible as we think. In many rural parishes there are no medical facilities that offer this service, and those which do can be expensive. Therefore, in many instances, women are forced to travel outside their parish to access the services," Spencer highlighted.
The cost to access mammograms is cheaper in public facilities, but the only public facilities which house mammography machines are the country's three Type 1 hospitals — The University Hospital of the West Indies, the Kingston Public Hospital (both in the Corporate Area), and the Cornwall Regional Hospital in St James.
The distance for women who do not live in these parishes makes access limited, while to get the procedure done at private facilities, they could pay as much as $12,000 for a mammogram.
"This is why two years ago we introduced this initiative, and last year, the offer was oversubscribed. Therefore, there is a high demand, and so we have maintained this offer to provide more women with a chance to prevent the disease by knowing their status," she pointed out.
The Power of Pink, being initiated this year under the theme 'Take the Brave Steps', will centre on encouraging women to conduct regular self-examinations and to get screened, so the disease can be detected early and treated to reduce deaths.
"Many women, and men too, fear receiving the news of a positive diagnosis, but by knowing their status early they can overcome the disease," Spencer assured.
She added that, as in past years, the campaign will be used to draw attention to and honour people battling the disease, as well as those who fought it bravely to the end.
"We will be celebrating the lives of warriors and remembering our heroes who have passed. Our campaign is targeted at educating Jamaicans about early detection and raising funds for cancer research and support for persons affected by the disease," she explained.
She noted that throughout October, the group will be supporting the cause through several of its various member companies.
"Beyond the need for early detection, we will highlight through our member companies the socio-economic challenges persons battling the disease face, and their stories of hope and survival," Spencer outlined.
She said persons may visit the JN Group website www.jngroup.com/pink/ to learn more about its activities in support of the fight against breast cancer and how they can participate.
Breast cancer is the leading cause of cancer-related deaths in Jamaican women.
Speaking at a JN Group Power Pink pop-up session held outside the JN Bank Half-Way-Tree branch in October 2022, Micheal Leslie, acting executive director of the JCS, said that "it is predicted that one out of every 21 women in Jamaica will develop breast cancer in her lifetime".
He also noted that 1,208 new breast cancer cases were diagnosed in 2020, which was an increase of more than 25 per cent when compared to 2018. Of the 1,208 cases, there was an estimated 637 breast cancer deaths, which he referred to as "alarming statistics".
Last year, the JN Group donated over $2.5 million to the JCS and its breast cancer arm, Reach to Recovery, to facilitate breast cancer research and support the fighters.
2 years 3 weeks ago
Child mental health and wellness KCNK 2023/2024 focus
NEWLY installed president of the Kiwanis Club of New Kingston (KCNK) Erica Haughton has charged members of the all-female club to join hands and hearts in addressing the poor mental health of children.
Speaking at the club's 35th installation ceremony held at Terra Nova All-Suite Hotel in St Andrew on October 7, Haughton said the focus stems from unresolved childhood trauma and the resulting troubling behaviours of youth.
"Added to the basic needs of food, clothing and shelter, our children need stable emotional and behavioural support systems to guide them into being productive and well-balanced members of society," Haughton said.
She added: "World Health Organization estimates that, worldwide, about 20 per cent of children and adolescents experience mental and behavioural disorders. Half of all mental illnesses begin by the age of 14 and are unidentified and untreated. I want to stress that children with mental health issues may struggle with low self-esteem, troubled relationships, and poor performance in school. They are the ones we hear about beating another child unconscious for something as simple as stepping on their shoe."
Keynote speaker, consultant psychiatrist Dr Geoffrey Walcott painted a picture of a history of mental health challenges from slavery into post-colonial society, explaining that the minute one begins to dehumanise a group of people it leads to atrocities, much of which are still being played out in today's society.
He further highlighted that most of the uncontrollable behaviour seen in children can be easily diverted, but "they don't end up in the child guidance clinic because nobody recognises bad behaviour as a mental illness, which it is".
"Children, particularly those who are depressed, do not present and tell you that they are sad. [Instead], they punch somebody in the face and box down a boy because him step on him shoes - that's how depression presents in children. But do they get referred?" Dr Walcott questioned.
For the 2023/2024 administrative year KCNK will lend support to the child guidance clinic at the Comprehensive Health Centre in Kingston, as it embarks on an ambitious undertaking to train teachers and other community leaders to recognise and treat with the manifestations of mental health disorders.
2 years 3 weeks ago
Health Archives - Barbados Today
Teen with rare disorder recovering and heading to Barbados
Second-generation Barbadian Daniella Sawyers is enjoying a new lease on life at 17 and will soon be granted her wish – to visit Barbados.
Second-generation Barbadian Daniella Sawyers is enjoying a new lease on life at 17 and will soon be granted her wish – to visit Barbados.
She was diagnosed with Rett syndrome – a rare genetic neurological and developmental disorder that affects the way the brain develops, and causes a progressive loss of motor skills and language – at the age of two, when she began showing signs of unsteadiness and could not stand or walk for long periods of time.
In June, she began treatment at Cohen Children’s Medical Centre with a newly approved drug that dramatically reduced the symptoms of her illness.
Daniella was present at a press conference on Tuesday, at which her doctor, Sanjeev Kothare, MD, director in the Division of Pediatric Neurology at Cohen Children’s Medical Centre, presented his findings.
Also present, along with her Barbadian mother Chyrel, her Jamaican father Donovan and other members of the Northwell Health team, were Consul General of Barbados at New York Mackie Holder, and Deputy Director, Barbados Tourism Marketing Inc. (BTMI) USA, Tenisha Holder.
Rett syndrome occurs almost exclusively in girls and leads to severe impairments that affect nearly every aspect of the child’s life, pointed out Dr Kothare, who has been treating Daniella for the past few years. The disorder is caused by mutations on the X chromosome on a gene called
MECP2.
It is estimated that Rett syndrome occurs worldwide in one out of every 10 000 female births. Patients will live to middle age or beyond with increasingly debilitating symptoms if not treated.
By the time Dr Kothare started treating Daniella in 2021, she was experiencing chronic and uncontrollable seizures – as many as 30 to 40 in one day – and her ability to speak was very limited. Her mother said that Daniella “spoke with her eyes”.
That began to change when Dr Kothare prescribed a drug called Daybue (trofinetide), which was approved by the FDA in March. The new drug improved cognition, gait and behaviour.
We are so grateful to Dr Kothare for prescribing Daybue for Daniella,” said the teen’s mother. “In just three months, she is walking and speaking sentences. And the seizures are much less frequent and of shorter duration. The thing to remember is that children like Daniella understand everything – it’s like they’re trapped inside a piece of glass.
According to Dr Kothare, Daniella will be taking the medication for the rest of her life. He believes that she and her family will continue to see improvements.
The Barbados representatives were part of the event after a Northwell representative contacted Consul General Holder about Daniella’s condition and her wish to visit Barbados, the birthplace of not only her mother but of Rihanna, of whom she is a big fan.
When Holder heard, he sprang into action. The family and audience burst into applause when he announced that the Sawyers family would be treated to a one-week vacation in Barbados.
Daniella clearly understood the announcement. Looking at her mother, she said, “I love it.”
Holder said it was an honour to have Barbados associated with the announcement of the medical breakthrough by Northwell, which has been particularly kind to the island during the COVID-19 pandemic and with which he had built a strong relationship.
He noted that the Consulate could not help but get involved when he heard of Daniella’s story. He said making her dream trip come true was a reflection of the DNA of Barbados which has built a reputation for warmth and hospitality, whether sharing a meal with strangers or giving refuge to stranded persons and ships, as it did during the pandemic.
He also pointed out that Barbados was known as a place people visited for its recuperative climate.
Tenisha Holder said BTMI was happy to facilitate the family trip to Barbados and would ensure Daniella sees Rihanna’s childhood home and enjoys as much of what the island has to offer as possible.
The post Teen with rare disorder recovering and heading to Barbados appeared first on Barbados Today.
2 years 3 weeks ago
A Slider, Charity, Health

Health Archives - Barbados Today
Daughter’s tribute to mum’s cooking
In the wake of a loved one’s passing, many find solace in preserving cherished memories through photos, mementoes, or keepsakes. For former journalist Krystal Penny Bowen, the route of memory for her late mother, Sheralene Bowen, begins in the kitchen. The destination is the book, Food: My Mother’s Love Language: Celebrating the Life of Sheralene Bowen, a culinary tribute encapsulating her mother’s delicious recipes.
Bowen has received heartwarming feedback from readers who commend her for the touching tribute to her mother.
She fondly recalled one of her most cherished memories of working side by side with her mother in the kitchen, a place where they not only prepared meals but also nurtured their bond.
“My mother loved to let me take photos of her food. I think that was the only way that I could be in the kitchen. In addition to that we would work together to get her food orders out. I was often called on to get the supplies or prep the raw materials. I would provide as much support as possible and in some cases, I would even serve the food at the event during her catering jobs,” she said.
The idea took root in November 2021 when Krystal created a 12-page draft containing her ailing mother’s 12 cherished recipes. Sheralene wholeheartedly embraced the concept and supported her daughter’s effort until she succumbed to cervical cancer just four months later. Krystal was determined to see her dream of publishing the book come to fruition, not only as a culinary compilation but also as a brief glimpse into the multifaceted life of her beloved mother, who was not only a chef but also a devoted mom and active community member.
Krystal emphasised her dedication to commemorating her mother’s life with the utmost respect for her final days and their family. The book primarily focuses on her mother’s remarkable career as a cook and entrepreneur, taking approximately four months to complete. Krystal collaborated with Robert Gibson of Passionate Words Editing Services, whose expertise was invaluable in shaping the book’s layout and appearance.
While the writing process was undoubtedly challenging, Krystal firmly believes it played an integral role in her healing journey by allowing her to share her mother’s incredible persona with a wider audience.
Krystal said: “My mother was an incredible person. She was artistic, funny, kind and loving. She was a social butterfly – she enjoyed socialising, dancing, singing and volunteering. As a cook and chef, she worked in hospitality, in food canteens as well as in several restaurants such as the now defunct BJ’s Café, Wonderland Deli and the University of The West Indies Cave Hill Campus Cafeteria. She catered for The University of The West Indies, Cave Hill Campus, World Cup 2007, QEH Medical Staff as well as for the late Prime Minister of Barbados, The Rt. Hon. David Thompson and then-Attorney General of Barbados, and now Prime Minister of Barbados, The Hon. Mia Amor Mottley. Mom was unable to work for many years due to her declining health, in 2022 she was diagnosed with advanced cervical cancer.”
The graduate of The University of Leicester with a Masters of Art in Media, Communications, and Public Relations urges others to consider documenting their loved ones’ legacies through writing, as it can provide solace during the grieving process.
“Writing a book about your loved one is difficult, but I believe one should do it. My mom meant the world to me. She was my friend, she loved me unconditionally. When writing, think of what was truly special about that parent. For my mother, it was her love of cooking and how she used food to share her love. Food was her love language –it was how she showed her feelings, and she was an incredible cook too,” she shared, encapsulating the profound sentiment behind her tribute to her mother. (PR/BT)
The post Daughter’s tribute to mum’s cooking appeared first on Barbados Today.
2 years 3 weeks ago
A Slider, Health, lifestyle, Living Well, Local News
The breast cancers that DON'T start with a lump: Two survivors of rarer subtypes of disease issue warning to other women about symptoms that doctors nearly missed
Olivia Franz (right) and Meadow Bailey (left) survived subtypes of breast cancer and are issuing a warning to others to be on the lookout for less obvious signs of the disease.
Olivia Franz (right) and Meadow Bailey (left) survived subtypes of breast cancer and are issuing a warning to others to be on the lookout for less obvious signs of the disease.
2 years 3 weeks ago
Medical News, Health News Latest, Medical News Today - Medical Dialogues |
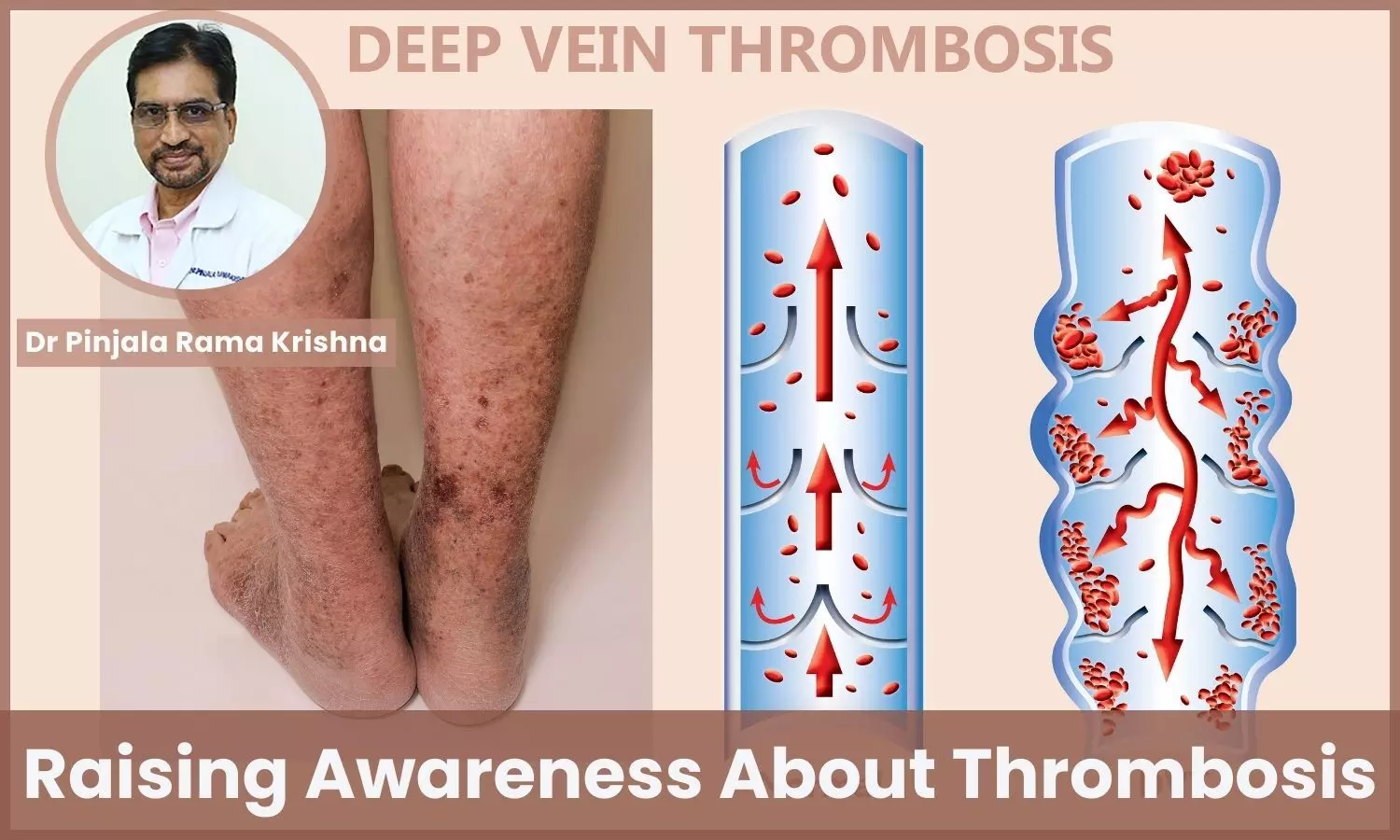
World Thrombosis Day: Raising Awareness and How to Prevent Blood Clots? - Dr Pinjala Rama Krishna
Healthcare
professionals worldwide should be acutely aware of the risk of blood clots in
clinical settings. Blood clots, particularly deep vein thrombosis (DVT) and
pulmonary embolism (PE), together with venous thromboembolism (VTE), pose a
significant health threat to patients. These potentially life-threatening
Healthcare
professionals worldwide should be acutely aware of the risk of blood clots in
clinical settings. Blood clots, particularly deep vein thrombosis (DVT) and
pulmonary embolism (PE), together with venous thromboembolism (VTE), pose a
significant health threat to patients. These potentially life-threatening
conditions can manifest silently and without warning, making vigilance and
knowledge crucial.
Healthcare providers should recognize the risk factors, which
include prolonged immobility, surgery, trauma, cancer, and certain medications,
among others. Timely risk assessment, prophylaxis, and early detection are
essential components of preventing thrombotic events.
Moreover, understanding
regional and patient-specific factors that may influence clotting risk is
paramount, as individual susceptibility can vary. By staying informed about the
latest research, guidelines, and preventive strategies, healthcare
professionals can play a pivotal role in reducing the global burden of
thrombosis-related morbidity and mortality.
World
Thrombosis Day, a global campaign of the ISTH, provides healthcare
professionals with up-to-date scientific research, news and clinical
recommendations.
I am a vascular
surgeon who works with patients who have different types of blood clots. At an
early age, I realized that I wanted to be a doctor and it stuck with me
throughout my years in school. I have been fortunate to work with many
physician role models and mentors.
I am very happy with where I ended up as a vascular surgeon, who takes care of blood clots in patients. My patients with
blood clots are my true motivators to do this work on this subject every day
and be a part of caring and treatment teams to improve the health of VTE.
DVT/PE patients which is very rewarding.
Blood clots
can either be provoked or unprovoked. Provoked blood clots are associated with
known risk factors, while unprovoked are those where no obvious risk factor can
also be identified. Most blood clots diagnosed are provoked, the commonest
cause being recent hospital admission.
Venous
thromboembolism (VTE) can affect men and women of all ages, races and
ethnicities. People at the highest risk (e.g., people admitted to
hospital, especially those with cancer, having surgery, or with major trauma
and/or immobilization) should receive preventative treatments. So people
admitted to the hospital should ask about their need for VTE prevention.
Blood clots
can affect anyone regardless of location, age, ethnicity or race. The most
important thing you can do to protect yourself from a life-threatening blood
clot is to learn if you are at risk. Know the signs and symptoms and contact
your healthcare professional immediately if needed.
The signs and symptoms of a blood clot, as well as the recommended
treatment, hinge on the location within your body where the clot forms and the
potential harm it might inflict. Deep vein thrombosis (DVT) typically manifests
with symptoms such as swelling, pain, warmth, and redness in the affected limb.
On the other hand, pulmonary embolism (PE), can present with chest pain,
shortness of breath, and rapid heart rate, and in severe cases, it can be
life-threatening.
Collectively known as venous thromboembolism (VTE), DVT and PE are
conditions in which blood clots develop within veins. While these symptoms may
vary, prompt diagnosis and appropriate treatment are vital for preventing
complications and ensuring the best possible outcome. Recognizing the signs and
symptoms of VTE is crucial, as it empowers individuals to seek medical
attention promptly, potentially saving lives.
Prompt treatment may be life-saving Treatment of blood clots can differ by the patient but typically
includes blood-thinning medication to prevent new clots from forming. There are
three main treatment goals:
1). Prevent the clot from getting bigger.
2). Prevent
the clot from breaking loose and travelling to the lungs.
3). Reduce the chances
of reoccurrence.
Please talk to your healthcare professional about the best
treatment plan for your unique health needs. For an overview of treatment
options, continue reading below.
Disclaimer: The views expressed in this article are of the author and not of Medical Dialogues. The Editorial/Content team of Medical Dialogues has not contributed to the writing/editing/packaging of this article.
2 years 3 weeks ago
Health Dialogues
PAHO/WHO | Pan American Health Organization
Dr. Rhonda Sealey-Thomas, a citizen of Antigua and Barbuda is sworn in as PAHO/WHO Assistant Director
Dr. Rhonda Sealey-Thomas, a citizen of Antigua and Barbuda is sworn in as PAHO/WHO Assistant Director
Oscar Reyes
12 Oct 2023
Dr. Rhonda Sealey-Thomas, a citizen of Antigua and Barbuda is sworn in as PAHO/WHO Assistant Director
Oscar Reyes
12 Oct 2023
2 years 3 weeks ago
Stay hydrated by eating water-rich fruits and vegetables
“One can also stay hydrated in extreme heat by consuming water-rich fruits and vegetables that can be found in the backyard or in the market”
View the full post Stay hydrated by eating water-rich fruits and vegetables on NOW Grenada.
“One can also stay hydrated in extreme heat by consuming water-rich fruits and vegetables that can be found in the backyard or in the market”
View the full post Stay hydrated by eating water-rich fruits and vegetables on NOW Grenada.
2 years 3 weeks ago
Education, Health, lifestyle, PRESS RELEASE, gfnc, grenada food & nutrition council, grenada food and nutrition council, heat wave, world food day

KFF Health News' 'What the Health?': Health Funding in Question in a Speaker-Less Congress
The Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
As House Republicans struggle — again — to decide who will lead them, the clock is ticking on a short-term spending bill that keeps the federal government running only until mid-November. The turn of the fiscal year has also left key health programs in limbo, including the one that provides international aid to combat HIV and AIDS.
Meanwhile, a major investigation by The Washington Post into why U.S. life expectancy is declining found that the reasons, while many and varied, tend to point to a lesser emphasis on public health here than in many peer nations.
This week’s panelists are Julie Rovner of KFF Health News, Sarah Karlin-Smith of the Pink Sheet, Victoria Knight of Axios, and Lauren Weber of The Washington Post.
Panelists
Sarah Karlin-Smith
Pink Sheet
Victoria Knight
Axios
Lauren Weber
The Washington Post
Among the takeaways from this week’s episode:
- House Republicans are choosing a new speaker with government funding still uncertain beyond Nov. 17. But some programs are already experiencing a lapse in their congressional authorizations, notably the global HIV/AIDS program known as PEPFAR — and the problems in renewing it are sending a troubling signal to the world about the United States’ commitment to a program credited with saving millions of lives.
- Drug companies have entered into agreements with federal health officials for new Medicare price negotiations even as many of them challenge the process in court. Early signals from one conservative federal judge indicate the courts may not be sympathetic to the notion that drug companies are being compelled to participate in the negotiations.
- Kaiser Permanente health system employees and pharmacists with major chains are among the American health care workers on strike. What do the labor strikes have in common? The outcry from workers over how staffing shortages are endangering patients, leaving overwhelmed medical personnel to manage seemingly impossible workloads.
- Elsewhere in the nation, new covid-19 vaccines are proving difficult to come by, particularly for young kids. Officials point to this being the first time the vaccines are being distributed and paid for by the private sector, rather than the federal government.
- Reporting shows those getting kicked off Medicaid are struggling to transition to coverage through the Affordable Care Act exchanges, even though many are eligible.
Also this week, Rovner interviews physician-author-novelist Samuel Shem, whose landmark satirical novel, “The House of God,” shook up medical training in the late 1970s. Shem’s new book, “Our Hospital,” paints a grim picture of the state of the American health care workforce in the age of covid.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week that they think you should read, too:
Julie Rovner: The Atlantic’s “Virginia Could Decide the Future of the GOP’s Abortion Policy,” by Ronald Brownstein.
Sarah Karlin-Smith: The Wall Street Journal’s “Children Are Dying in Ill-Prepared Emergency Rooms Across America,” by Liz Essley Whyte and Melanie Evans.
Lauren Weber: ProPublica’s “Philips Kept Complaints About Dangerous Breathing Machines Secret While Company Profits Soared,” by Debbie Cenziper, ProPublica; Michael D. Sallah, Michael Korsh, and Evan Robinson-Johnson, Pittsburgh Post-Gazette; and Monica Sager, Northwestern University.
Victoria Knight: KFF Health News’ “Feds Rein In Use of Predictive Software That Limits Care for Medicare Advantage Patients,” by Susan Jaffe.
Also mentioned in this week’s episode:
- The Washington Post’s “Medicaid Rolls Are Being Cut. Few Are Finding Refuge in ACA Plans,” by Amy Goldstein.
- The Washington Post’s “An Epidemic of Chronic Illness Is Killing Us Too Soon,” by Joel Achenbach, Dan Keating, Laurie McGinley, Akilah Johnson, and Jahi Chikwendiu.
- The Washington Post’s “How Red-State Politics Are Shaving Years Off American Lives,” by Lauren Weber, Dan Diamond, and Dan Keating.
- The Washington Post’s “England Considers Raising Smoking Age Until Cigarettes Are Banned Entirely,” by Andrew Jeong.
click to open the transcript
Transcript: Health Funding in Question in a Speaker-Less Congress
KFF Health News’ ‘What the Health?’Episode Title: Health Funding in Question in a Speaker-Less CongressEpisode Number: 318Published: Oct. 12, 2023
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello, and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, Oct. 12, at 10 a.m. As always, news happens fast, and things might’ve changed by the time you hear this, so here we go.
We are joined today via video conference by Victoria Knight of Axios.
Victoria Knight: Good morning.
Rovner: Sarah Karlin-Smith of the Pink Sheet.
Sarah Karlin-Smith: Hi, everybody.
Rovner: And Lauren Weber of The Washington Post.
Lauren Weber: Hello, hello.
Rovner: Later in this episode, we’ll have my interview with doctor-author Samuel Shem, who wrote “House of God,” the seminal novel about medical training, back in the 1970s, and who has a new take on what ails our health care system. But first, the news. So, we’ve been off for a week so KFF could have an all-staff retreat in California, which was lovely, by the way. And against all odds, it’s Oct. 12 and the federal government is not shut down, although the continuing resolution that squeaked through Congress at the very last minute on Sept. 30 expires Nov. 17, so we could be going through all of this again next month.
Meanwhile, conservative Republicans, who were angry that House Speaker Kevin McCarthy agreed to keep the government open, ousted him from his job, the first time ever a speaker has been kicked out mid-Congress, and things are, to put it mildly, in disarray. But I want to go back to that six-week continuing resolution. It does just continue appropriations, but it also had some important, if temporary, authorizing provisions, like for community health centers, right, Victoria?
Knight: Yeah, that’s right. There were a few provisions that just kind of kept it going as it was, funded at the same level. That was community health centers, and there were a few for the Pandemic and All-Hazards Preparedness Act. Then there were also some things that were not renewed in PAHPA, and then also the PEPFAR program [the U.S. President’s Emergency Plan for AIDS Relief], which I figured we might talk about a little bit, which is the program that funds programs in other countries to help with HIV/AIDS treatment and research, and it’s been a long-standing bipartisan program, and it has come up against some obstacles this Congress.
Rovner: Just to remind people who don’t follow this as closely as we do, the appropriations are what actually keep the lights on. Those are the spending bills that Congress has to pass, either in permanent or temporary fashion, at the beginning of the fiscal year, Oct. 1, or things shut down. Things like PEPFAR and community health centers continue to get funded, but their official authorizations expired at the end of the fiscal year. While the community health centers were kept going, PEPFAR has not. Of course, the House, which is, as we speak, still leaderless, can’t really do anything. Are there, at least, negotiations going on? I know PEPFAR really is a bipartisan program, as you say, and there is some effort to keep it going, because some people frankly say it’s embarrassing for the United States to look like it is reneging on this, even though it’s technically not.
Knight: Well, I know it was originally started under a Republican president, George W. Bush, and has always been reauthorized for five-year intervals. That’s never not happened. I’ve talked to members of Congress about this. In the House, they only want to reauthorize it for one year, and they’ve been very open about that’s because they want a new Republican president to come in and further restrict where funding is going, to really, in their mind, ensure it’s not going to abortion funding, even though there’s really no evidence that funding from PEPFAR goes to NGOs [nongovernmental organizations] that fund abortions or anything like that.
Then, in the Senate, it’s a different story. Another little factor is that Sen. Bob Menendez was the lead on this, and then he had to step —
Rovner: Oops.
Knight: He had to step down from his chair of the Senate Foreign Relations Committee, and that’s just a matter of Senate rules, since he’s under indictment.
Rovner: Again.
Knight: Again, yes, and so Sen. Ben Cardin just took that chairmanship. I’m not sure how much PEPFAR is on his radar. I tried to ask him about it recently, and he was like, “I’ve got to go to a meeting.” I know for Menendez, it was a really big thing that he cared about and was like, “I want to reauthorize it for five years.” So, as far as I can tell, it’s kind of a standstill between the House and the Senate and, to be determined, but maybe at the end of the year, if we get a big bill, something will be put in there. Maybe they’ll negotiate it to three years. I’ve heard something about that, but again, this will be the first time it hasn’t been reauthorized for five years, and that would send a signal to other countries that maybe the U.S. is not as devoted to treating HIV/AIDS and helping programs in other countries.
Rovner: Yeah, obviously, with everything else going on in the world, it’s not the biggest deal, but there are still a lot of people who are very concerned about it. The other at least somewhat surprising thing that happened on Oct. 1, the beginning of the fiscal year, is that all of the drugmakers responsible for the 10 drugs that Medicare has selected for the first round of price negotiation have agreed to negotiate, at least for now. That’s likely because the first round of the first of several lawsuits in federal court seeking to block the program found in favor of the government. In other words, the program did not get blocked by the courts. But Sarah, this fight is a long way from over, right?
Karlin-Smith: Yeah, there’s a number of lawsuits. I think we might be up to eight now, but don’t hold me to that exact figure.
Rovner: Excel spreadsheets.
Karlin-Smith: Yeah. Even this lawsuit, the initial blow I think was pretty big for the drug industry here, because we have a Trump-appointed judge who made a pretty clear preliminary decision that he doesn’t think the drug industry can make its constitutionality challenges that this law is not constitutional, which I think is a pretty big deal, because most of the initial lawsuits revolved around constitutional challenges. Then, there are other issues, in the first particular case, around whether even the people who are suing have standing or it’s ripe for a lawsuit now, whether because anybody’s actually been harmed at this point. Yet, everybody, all the companies, have entered into agreements with Medicare to negotiate now. A lot of them have said, “Well, we’re doing this, but basically because we have no other choice. We have to. We’re doing it in protest. We’re still continuing our lawsuits.”
So, you can expect two parallel tracks to be going on right now, mostly behind the scenes. This is pretty much going to take a whole year for Medicare and the companies to get to the place where we’ll then see a public negotiated price next fall, next September. And these lawsuits to proceed, again, just I think the constitutionality issue got a really big blow. There are some other lawsuits that I think could be more interesting that are arguing more about decisions Medicare made, so more about APA, Procedures Act, cases, which are a little bit different and I think might have a little bit more chance of getting the drug industry some wins.
Rovner: The APA is the Administrative Procedures Act —
Karlin-Smith: Procedures Act, thank you.
Rovner: — and basically saying that Medicare didn’t follow all of the appropriate rules in how it devised and rolled out the program.
Karlin-Smith: Right, and I think —
Rovner: As opposed to the big lawsuits that said, “You can’t force us to do this,” which, not a lawyer, but every other health provider goes under the if you want to play in Medicare, you have to take our price, so it’s hard to see where the drug companies are going to have something completely different, but that’s just me. You never know.
Karlin-Smith: Right, and this Trump-appointed judge — I keep emphasizing that because they picked the 5th Circuit, they looked for a friendly judge, and they couldn’t get the win there. He said, “Medicare is a voluntary program. The government has stopped forcing you to participate in Medicare. If you don’t like this, you can leave.” I think this is a pretty symbolic loss for the industry and some of these arguments they’re going to make.
That said, these APA cases, you can maybe see them getting more tweaks around the edges to shift the program in ways that favor it, but we know the way litigation works in this country; it’s going to be this long slog to figure out how that shakes out as the program is potentially, again, on the other side, getting worked out and maybe implemented.
Rovner: We will see. All right. Well, elsewhere in disarray, if this was the summer of strikes in Hollywood, it’s shaping up as the autumn of strikes by health workers. Last week, 75,000 workers at Kaiser Permanente — no relation, just for my listeners — in several states walked out for three days. Workers at several other hospitals in and around Los Angeles walked out, and we’re seeing pharmacists taking work actions at both of the big chains, CVS and Walgreens. All of these walkouts have basically the same thing in common. Striking workers say that the shortage of personnel is endangering patients, as those who are left at work face impossible workloads.
These employers are not in a great situation to fix this. Covid accelerated the departure of a lot of healthcare workers, and there simply aren’t the bodies to fill all of these vacant positions. Is there any settlement in sight? Any way to fix any of this that anybody’s proposed?
Weber: I think if any of us sitting at this table have family, friends that work as nurses or pharmacists, they’ve been hearing about these problems for years. I mean, all it takes is talking to somebody that works in this industry to realize that they have been short-staffed and underfunded for a very long time. A lot of them really worry about the actual errors that can result from that. I mean, I think what’s really important to consider is to get to a strike, you have to have a lot of bad things going on. I mean, I think some of the reports say that some of these hospitals have filed countless complaints with the local county health in California that had not gotten listened to about their staffing shortages.
When you have short staffing for nurses, that means that you feel like patients are not getting seen. Something could be happening. They feel like they’re putting these people in jeopardy. I don’t really think there’s going to be a lot of end to this in sight. I think, once you kick off these strikes like this, it’s a bit of a chain effect. I mean, we saw CVS pharmacy employees had a strike, and then Walgreens employees have started doing that.
Frankly, the CVS one was pretty successful. The CVS CEO went out there and said, “Look, we hear your conditions. We’ll work on cutting down hours, and we’ll try and accommodate you.” I think we’re going to be in for a lot more of these in the months to come.
Rovner: Yeah, I mean, it’s one thing if workers — there aren’t enough checkers at the grocery store and you have to stand in line for longer, but it’s quite another thing when you have a nurse in an intensive care unit trying to keep track of six patients instead of three or a pharmacist trying to keep track of basically everything that’s going on with no help. That’s what we’re seeing around the country with these shortages of trained health care workers.
In California, there’s another complication, because they actually have laws about patient-nurse ratios in hospitals, and some of them are not being actually obeyed, so I imagine that this is going to go on. We hear a lot about health care worker shortages. I think this is the worst one that I’ve seen in my career, where there just really aren’t the bodies to meet the demand here.
Well, speaking of things that also aren’t going swimmingly — that seems to be our theme this week — there’s a lot of early demand for the new covid vaccine that was approved in September, and apparently not a lot of supply. Also, as we just discussed, a lot of the responsibility for the vaccine is being pushed to pharmacies, whose already overstretched staff simply don’t have the bandwidth to deliver vaccines in addition to all the drugs that they’re asked to be counting out and prescribing. Sarah, shouldn’t the system have been more ready for this? It’s not like we didn’t know pretty much exactly when this vaccine was going to become available. They’ve been saying mid-September for the last five months.
Karlin-Smith: Right, yeah. I mean, there’s definitely been a lot of criticism, particularly on the health insurance side with the codes and things not being set up to put it in. It’s less clear exactly what has gone wrong in the supply chain issue, where there are reports of wholesalers not being able to get supply to the pharmacies. Do you even have enough shots? Lots of people are reporting they have appointments. They get there. They show up. The pharmacist is out.
One thing I’ve been wondering is just there’s been low uptake of boosters in the U.S., and so if it’s been harder for them to predict how much supply they want to have, it’s a bit different when the government is no longer funding those shots. Pharmacies, doctor’s offices have been concerned. What if they buy more than they end up using? Are they out money? I know, in some cases, some of the companies have made some concessions and said, “We will take back unused product,” and so forth, because there’s just different financial considerations that I think are impacting how much supply is on hand at different times right now.
Rovner: And, of course, it’s even worse for kids, right? Because kids can’t go, generally, to the pharmacies to get their vaccines.
Karlin-Smith: Right. Most of the country, to get a vaccine by a pharmacist, you have to be at least 3. It varies a little bit by state and so forth. A lot of pediatricians’ offices don’t have these shots. One of the reasons it seems to be is that, again, these wholesalers who ship the supply around the country have prioritized adult vaccinations. I know, personally, my pediatrician’s office still does not have a shot, as well.
Rovner: And you have two little ones, right?
Karlin-Smith: Right. Again, I have one under 3, and I looked into vaccines.gov the other day to see what would they tell me if I put in for an under-3-year-old. There was one pharmacy in all of D.C. that claimed they would vaccinate someone under 3 for covid, which, I haven’t done the legwork yet to see if that’s actually correct, but, you know, you’re hearing these reports of people traveling really far to get pediatric shots. Again, just to emphasize that there are babies being born all the time who, when they turn 6 months, they are getting their first covid shot, right? They have not, hopefully they haven’t, had covid. You want them protected before they get exposed, so that’s a really crucial gap in the health system that I think people don’t appreciate, because a lot of people are just thinking now, well, oh everybody’s had covid or had two or three shots, and this is a particularly vulnerable population that’s having trouble finding vaccines right now.
Rovner: Yet, I mean, considering it’s very early in the respiratory disease season, there seems to be a lot of covid going around right now, which I suspect is why there’s such a demand, at least among the people who are most concerned about getting the vaccine, for getting the vaccine. It feels like it did at the beginning, when it’s like suddenly there’s this big rush of people at the beginning who want it. Eventually, there’ll probably be more vaccine than is needed, but for right now, I mean, I’m seeing lots and lots and lots of stories and anecdotes and everything about people, as you say, making appointments, showing up, and having the pharmacy saying, “Oops, we didn’t get our supply.”
Karlin-Smith: I mean, there’s been this sort of hope and narrative that covid, is it going to become seasonal in the way we think of flu, where there’s generally a more clear, defined season? You can kind of make a good guess that the best time to get your flu shot is in October and know you’ll be protected all flu season. As much as we hope that’s the case with covid and eventually becomes the case, that’s really not true now. We’ve still had — again, they’re relative maybe compared to some other surges, but we’ve had surges pretty much every summer, so it’s been really difficult. A lot of parents, I think, wanted to get their kids vaccinated before they went back into school and classrooms. If you have little kids, you just know, it becomes a big germ bath, and everybody gets sick.
Rovner: And parents wanted to get themselves vaccinated before their kids went back to school and brought home those germs.
Karlin-Smith: Right, so the timing of it, again, hasn’t been great, for that regard, but I think it is just this difficulty with covid, in that we haven’t had that same predictability of when you might get it during the year, so it is a lot harder to protect yourself.
Rovner: We’ll see how that sorts itself out. Well, keeping with our continuing theme of things that are not going great, let’s talk about the Medicaid unwinding. Our podcast colleague, Amy Goldstein, has a troubling story in The Washington Post about how people whose Medicaid coverage is being canceled but who are eligible for subsidized plans under the Affordable Care Act are in fact having trouble making that transition. Sometimes people are falling through the cracks because states don’t have enough information to know what they’re eligible for or they don’t have the staff to process the transitions.
Sometimes in states like California, people fail to follow up, even when they are given all the information they need. Is this just the inevitable fallout of trying to redetermine the complicated eligibility rules for more than 90 million Americans in a single year, or could something more have been done? I mean, how many times did I hear them say, “It’s OK if you get dropped from Medicaid. We’re going to get you onto your Affordable Care Act plan that’s fully subsidized.” That doesn’t seem to be happening in every state.
Karlin-Smith: I mean, it seemed like, from Amy’s reporting, that there are some states that have connected their Medicaid systems and their exchange sign-ups really closely, and those are going better, but —
Rovner: California, yeah.
Karlin-Smith: Right. Yeah, she mentioned the Medi-Cal system, but then even these states that she calls out as the success stories still have fairly low transition rates. It’s just one of the many examples of our country of having such separate systems and very different bureaucratic processes for sign-up that really hurt people. As we’ve seen with this Medicaid process, a lot of it is just about these paperwork, if you will, call them burdens, that really get people to lose their health insurance and not be covered, so that’s really —
Rovner: I taped a podcast earlier this week aimed at young adults, teaching them how to quote-unquote “adult,” talking about health insurance and open enrollment and how to get signed up. After the Affordable Care Act, there are so many more protections than there were before, and yet it is still unbelievably complicated to try to explain to somebody who’s facing this for the first time. There are just so many possibilities and so many ways. There’s lots of ways to get health insurance, and there’s even more ways to fall through the cracks and not get health insurance. It seems that the more we try to put band-aids on the system, the more confusing it gets to everybody. Maybe I’ve been doing this for too long.
All right, well, finally this week, also in not great news, The Washington Post has published a giant project on declining life expectancy in the United States. It turns out the problem is a lot more complicated than just covid and drug overdoses. Those are the things we’ve been hearing about for a while, although those are indeed a piece of it. Lauren, you were part of the team that put this project together. Tell us the real reasons why Americans aren’t living as long as they used to and aren’t living as long as people in other countries.
Weber: Our team found that income had a big, big part to do with that. The poorest counties in the U.S., compared to the richest counties of the U.S., are doing 6 times worse than they were 40-some years ago, when it comes to life expectancy. The income gap has increased, obviously, but not nearly as much as the life expectancy gap has increased. I think that says something about the U.S.
In general, I mean, as you mentioned, a lot of people consider opioids, deaths of despair, to be what’s killing Americans across the country, but they’re really overlooking chronic illness. Our reporting, my reporting with Dan Diamond and Dan Keating and I, we looked at how the politics also play into life expectancy. What we found is that public health initiatives and public health laws, like tobacco laws for tobacco taxes, seat belt laws, and investing in public health, does have a direct correlation to longevity of life.
State politics and state policies and lawmaker decisions can shave years off of Americans’ lives. What we found in our reporting and in our analysis is that that was happening in red states, particularly those in the South and the Midwest. What we did is we compared three counties that ring Lake Erie: Ashtabula, Ohio; Erie County, Pennsylvania; and Chautauqua, New York. These three counties, they’re all pretty down on their luck. Industrially, the jobs have gone. None of these counties is a success story in health, but they’re all across state lines. It’s just very vivid to see how the different tobacco taxes, seat belt laws have resulted in totally different outcomes when it comes to life expectancy. And you could see, even reflected in these counties, the covid death rates tracked the state investments in public health and the state infrastructure in public health.
So, you know, something that our series looks to do is explain why a state like Ohio has the same life expectancy as Slovakia. One in 5 Ohioans won’t make it to 65. That’s a pretty wild stat. I think a lot of people in this country don’t realize that life expectancy, some of these preventable diseases are preventable.
Rovner: Yeah, I mean, I was really taken by the comparison of tobacco taxes. Where the tobacco taxes were the lowest, which I guess was Ohio, the rate of smoking and, surprise, smoking-related diseases was much higher, and therefore life expectancy was much lower. I noticed The Washington Post had yet another story this week, not quite the same, but how Great Britain and some other countries in Europe are trying to effectively ban smoking, not by banning it outright, which will just make it a black market, but by doing it year by year so that the current cohort of people who smoke will be able to continue but as younger people get older, it will become illegal, until eventually, when everybody dies off, smoking will be basically banned in Great Britain. Somehow, I can’t see that ever happening here, but it’s certainly a public health initiative that’s pretty bold.
Weber: It’s pretty bold. It would not happen here. I mean, look, one of the legislators that we talked to in Ohio, who had stopped a lot of the tobacco taxes — Bill Seitz, House floor majority leader for Ohio — he smoked for 50 years before he quit this summer, actually, because he got kidney cancer and lost a kidney, so he stopped smoking. But what he said to us, when we asked him how he felt about having blocked all these tobacco taxes and if he planned to keep doing that, he said, “Well, just because I quit smoking doesn’t mean I’m going to become a smoke Nazi now. People have the liberty and the right to smoke.”
I mean, a lot of what our reporting came down to is this concept of personal freedom and liberty versus public health, looking at the community as a whole. It was really fascinating to dig into some of the interesting dynamics in Ohio, especially because Gov. DeWine, who is a Republican, has been more bold on public health and has tried to push the legislature to consider more of these initiatives, in part because he has a personal story. His daughter died over 30 years ago in a car accident, and so he’s been very aggressive in especially car safety, but really in a lot of public health initiatives because, as he told us, that kind of death clarifies things for you when it comes to tipping the scales for people’s loved ones. We’ll see that dynamic play out across the U.S., but it is fascinating to examine how tobacco is very much with us. I mean, 20% of Ohioans smoke. I mean, this is not — I think a lot of people consider opioids and these things to still be the new thing to focus on, but tobacco cessation is still very much a fight happening across the country.
Rovner: It’s interesting to me that it’s not just — I mean, the shorthand is red versus blue, but it’s not really just red versus blue because, as you point out, Gov. DeWine’s a Republican, fairly conservative Republican. Before him, Gov. Kasich, also fairly conservative, or used to be considered a fairly conservative Republican. I mean, it’s really about being pro-public health or anti-public health. It gets us back to PEPFAR, right? Victoria, in the early 2000s, Republicans were very pro-public health. Newt Gingrich led the charge to double the funding at the National Institutes of Health. And these days, what you have are very conservative Republicans who apparently don’t believe in public health or in science.
Knight: I was going to say, I think what this series does so well is it emphasizes that so much of our challenges in the U.S. with health is not about the medical system of health; it is the things that we sometimes don’t even think about as health care, not even just public health, but the economic practices, our labor practices, our housing, our food system, that actually these are some of the main things that end up impacting who is living longer and healthier, and so forth. I actually did an interview with an outgoing pharma lobbyist this week, and she was saying — she mentioned chronic diseases, which was a big part of Lauren’s story, and saying, “We actually have more problems with chronic disease now than we did when I started, even though now we have all these cheap, generic medicines for, you know, we have statins and blood thinners and a lot of diabetes medicines that are generic and all these things.” Yes, we have problems with people accessing this medical system and affording it in the U.S., and that’s a big thing, but a lot of this is starting way before you get to the hospital and the doctor’s office, and the U.S. has all these amazing technologies, but we’re failing on these much more basic solutions to keeping people healthy and alive.
Rovner: It’s also not just physical access to health care. I mean, Ohio’s the home of the Cleveland Clinic, for heaven’s sakes, one of the major health care providers in the country. Many parts of Ohio are pretty rural, but it’s not like people have to drive hundreds of miles to get health care. I mean, this whole public health issue is not simply a matter of people can’t get to the doctor, the way we have concerns about that in places like Texas and the Far West. I mean, it really is just these everyday things, whether you wear your seat belt, whether you start smoking. I think it kind of shined a light on actual public health and the importance of public health to life expectancy.
Knight: I think, also, just going back to the politics of it for one second, I mean, I think the result of some of this is just the increased polarization between the two parties, and Republicans also, I think, were really mad about some decisions made during covid, and so we’re also seeing that where they’re, at the state and local level, wanting to strip money from public health departments, as Lauren has reported on at KFF Health News and the Post, and then that’s also, you’re seeing that in Congress as well, now, where they’re not wanting — they’re angry at some of these decisions made, and they want to strip funding from the CDC. They want to strip it from the NIH. We don’t know how the appropriations bills are going to end up, but it’s definitely something that they’re talking about in the House, at least, which is in Republican control.
Karlin-Smith: Everybody I talk to about anti-vaccine sentiment, they say once these sort of sentiments become aligned with your political identity, it makes it so much harder to shift course, so again, this idea that there’s political alignment around how we think about public health is just seen as so problematic because of how people see their identities. It becomes much harder to change people’s opinions when it’s tied into your politics like that.
Weber: Yeah, and I just wanted to highlight, so one of the folks I met in Ashtabula, Ohio, was Mike Czup, who was a funeral home owner, who was 52 years old. What he told me is that a quarter of the people he buries are younger than him. I mean, that’s just a wild statistic; a quarter of the people he buries are younger than him. Honestly, he wasn’t even surprised. I mean, that was just the norm. That was the way of life. I think that’s what this series shines a light on is that people across the U.S. just assume that lung cancer, heart attack, stroke — that’s just what happens. But that’s not the case across the world. It doesn’t have to be the case, and in certain states it’s not the case. California has much better life expectancy than Ohio does, despite them both being on a very similar trajectory in the ’90s. It’s pretty stark findings.
Rovner: Yeah, it’s a really, really, really good series. We will link to it on the podcast page. All right, well, that is this week’s news. Now we will play my interview with Sam Shem, physician, author, and playwright, and then we will come back and do our extra credits for this week.
I am honored to welcome to the podcast Samuel Shem — not his real name, by the way. Dr. Shem shook up the world of medical training back in 1978, when he wrote a groundbreaking novel about his first year as a medical resident, called “House of God.” It was funny and sad and painted an altogether not very pretty picture of medical training in Boston at some of the nation’s most esteemed hospitals and medical schools.
He has spent most of the past five decades crusading, if I can use that verb, to “put the human back in health care.” Fun fact: My mom interviewed him for The Washington Post in 1985. Now Shem has a new novel called “Our Hospital.” It paints a funny and sad picture of the state of medical practice and the state of the American patient in the era of covid. It’s actually the fourth and final volume of his irreverent evaluation of the U.S. health care system. I spoke to Dr. Shem from his home office in upstate New York and started by asking him why he wanted to write a novel about covid.
Samuel Shem: I don’t know how much longer I’m going to be able to write. Nobody does, really. What I did is I said, “Someone has to write about what’s going on in a hospital, and we have to now talk about nurses.” I haven’t put them at the forefront until now, because they have done so incredibly much. I’m taking all the other books, the “House of God” books and others, and I’m bringing them all together like a family. I don’t have a big family, so I’m absolutely doing this with care and vehemence and also a lot of skill in shifting gears, so go read it.
Rovner: I sort of approached this with trepidation, because who wants to read a novel about covid? But, in the end, it’s a pretty optimistic book about what the future of medicine can be, which, forgive me, feels odd for a novel about covid and the possible end of democracy. Are you really that optimistic about America’s ability to cure what ails our health care system, or did you just get tired of writing depressing literature about the health care system?
Shem: Well, I am a crazy optimist, because I grew up in a time, like your mother, when things changed. They changed because we got out there and we were in the streets, and it changed. I was partly in the USA and partly on a Rhodes in Oxford. I think we just have to get together and try to stay together. What this book does: The doctors and the nurses come together, and that is an immense force. We can do this. That’s what I think. The best person in the book, that I have ever written, in some ways, were the women nurses.
Rovner: The heroes of this book are all women, doctors and nurses. You’ve obviously been roundly criticized for your portrayal of women in the original “House of God.” Is it just that you wanted to make it up, or do you really think that women are the future of fixing health care?
Shem: The future of anything. My wife, Janet Surrey, and I, we worked a lot a long time ago on male-female relationships. Women are a beacon of what men could do in medicine. You’ve got to have some kind of group that can get what we need.
Rovner: You’ve watched the evolution of medical practice in America for half a century now, the amazing advances and depressing depersonalization and corporatization. Which one is winning, at this point?
Shem: Well, both. The money — it’s hard to take money from people with so much money. It’s crazy. It’s insane. There are other models, in Australia and all that stuff. What’s happening, unfortunately, is that doctors are running. They’re saying, “I don’t want to do this anymore.” Sooner or later, with some giant people talking about it — doctors and nurses — it can’t go on. It really can’t go on.
Some of the things that I’m hearing: Doctors, they’re saying, “Well, in two years, I’m gone. I can’t do this anymore.” But we can’t do it alone. I can’t say it so more and more. I mean, I know a lot about this in various different jobs I’ve had. It’s got to be with doctors and nurses.
Rovner: What ties a lot of your writing together is the notion of burnout for medical professionals, which may be, as you mentioned, one of the biggest problems right now in U.S. health care. If you could wave a magic wand, what’s one thing that you could do that could help medical professionals, both doctors and nurses and everybody else who works in medicine, love their work again?
Shem: It’s terrible. Young doctors, they don’t know what to do, you know?
Rovner: I mean, do you worry that people won’t want to go into medicine because it’s now viewed as doctors particularly don’t have the community esteem that they used to? Health workers are in danger sometimes in their own workplaces. It’s not a great situation.
Shem: Yes, I think we became horrified when we went on our first medical school times that we were in the hospital. Right when the kids go into the hospital, it’s obvious. It’s really obvious. They’re seeing the house staff spending 80% in front of a computer to bill, so they can’t help but do it.
The problem is you’ve spent so much money and so much time. What the hell should I do? But there are people who are really paying attention to this. I don’t really do it in person too much, but in everything I say these kinds of things, so I think it might help.
Rovner: You’ve now influenced several generations of medical practitioners. Is there a single lesson that you hope you have imparted on all of them?
Shem: Yes. This is what I start my addresses with. I call it staying human in medicine, the danger of isolation and the healing power of good connection. It’s not I-you; it’s the connection that goes after each of them. What’s good connection? Mutual connection. If it’s not mutual, it’s not that good. If you let me, maybe I could read the very end. Is that all right?
Rovner: Yes, please.
Shem: “I’m with you totally. Almost everyone in medicine is hurting, doctors, nurses, and all the others, working in the money-driven hell realms of American care. We’re all suffering terribly. Covid has lit it all up for all to see. The resists to our bodies, minds, and spirits are profound, killing ourselves, acting normal, the poor and people of color dying in droves.”
He paused, scanning the trees for the fat man. Nothing. He went on, “We do miracles every day, we doctors, but we haven’t been able to get a place to work in body and spirit. One in 5 health care workers have quit. Many of us died. At the start of covid, we did the most important thing for us and our patients. We stuck together.” We did. It’s a model, right? But not lasting into the daytime. Hatred and money killed it. I have confidence. We’re no dopes, we docs.
I just think people like you, and people who pay attention, it’s inevitable. I do think it’s inevitable that we’re going to get better stuff. It really will.
Rovner: And get some of the greed out of medicine?
Shem: Yes, because it’s going to crash. You can’t go on like this. Nobody can go on like this. I think so. I really do. You know what? It doesn’t take much. How did we get rid of the presidents in the ’60s? Basically, people who are into power are scared about losing the power, you know, all of the people who protect them and all that stuff.
Rovner: Well, thank you very much, Dr. Samuel Shem. Thank you for joining us.
Shem: OK.
Rovner: We are back, and it’s time for our extra credit segment. That’s when we each recommend a story we read this week we think you should read, too. As always, don’t worry if you miss it. We will post the links on the podcast page at kffhealthnews.org and in our show notes on your phone or other mobile device. Victoria, why don’t you go first this week?
Knight: Sure thing. My extra credit is from KFF Health News, and it is called “Feds Rein In Use of Predictive Software That Limits Care for Medicare Advantage Patients,” by Susan Jaffe. This basically was looking at how Medicare Advantage plans, which are plans that private health insurers run for people that are of Medicare age — they’re basically running their health insurance programs — it’s talking about how these MA plans are using predictive software systems to make coverage decisions for patients, and so they’re looking at other patients that may have similar illnesses and what their treatments were and how long it took to treat them and then, based on that, deciding when they should cut off coverage for patients.
Rovner: That doesn’t always work very well, does it?
Knight: No, it does not. This story chronicles how this has happened to several patients, who were not ready to finish having whatever their treatment, illness — the person profiled in the story still couldn’t walk well. She had a colostomy bag, and they were going to cut off her coverage, and so she had to keep paying for it, almost $10,000, just because this software said, “Oh, you should be done by now, based on other people’s cases.”
But there is some good news, in that there is a Biden administration regulation that will be put into effect in January, and that’s going to do a better job of making sure these plans take the individual patient’s circumstances into account when making these coverage decisions, but we’ll see how that actually plays out. It takes effect in January.
Rovner: Really good story.
Knight: Yes, it’s a very good story, yes.
Rovner: Sarah.
Karlin-Smith: I looked at a Wall Street Journal story, “Children Are Dying in Ill-Prepared Emergency Rooms Across America,” by Liz Essley Whyte and Melanie Evans. It’s a piece that talks about how so many hospitals are not properly equipped to treat pediatric patients when they go to the ER. It’s a failure of regulations, standards, and so forth. They really document how this has been a long-known problem, going back 20-plus years, and things have not changed. This may mean that you might not — even if you have a hospital near you — you might not have a hospital that really can successfully save your child’s life. That is because children are not little adults. There’s different — you really have to be trained to know how to deal with them in emergencies and also even just have the equipment, the specialized sized equipment and so forth, to deal with them in emergencies.
It’s a really sad story. It gets into some of the economic reasons why these hospitals are not prepared. But again, it gives you a sense of a connection to Lauren’s piece, and the Post’s big piece, which is that we have a lot of tools and technology we’ve developed in this country, but if it’s not available to the people when and where they need it, lives don’t get saved.
Rovner: This piece really shook me, because I assume that — I mean, kids are the ones who seem to end up in the emergency room most often. They’re the ones who have accidents and fall off their bikes and get sick in the middle of the night and all those other things, and yet so many emergency rooms are not prepared for them. Anyway, Lauren.
Weber: I picked a piece that is particularly alarming if you know anyone that has a CPAP [continuous positive airway pressure] machine, but it’s titled “Philips Kept Complaints About Dangerous Breathing Machines Secret While Company Profits Soared.” It’s a collaboration between ProPublica, the Pittsburgh Post-Gazette, and Northwestern, and I believe a Netherlands paper, as well. It’s a very disturbing investigation about how Philips knew, had been getting a ton of complaints, that when they rejiggered some of their breathing machines, the foam was disintegrating and chunks of the black material was then getting into people who were using the breathing machine’s lungs and, from the court cases, it appears, causing them potential cancers and adverse health effects.
The FDA, I guess, from reading the piece, requires that companies report complaints, but according to this, Philips did not tell the FDA about all these complaints. It’s a really alarming story, because you’re like, how many other companies are not telling anyone about the complaints they’re receiving? Just really well-done investigation. It appears to be based on court documents, so hats off to them, but very disturbing, again, if you have anyone that has a CPAP or breathing machine they need to sleep, which is vital for everyone. If you have an understanding about how those work, you are hooked up to it, so you are forced to breathe through it, so it really disturbed me that that could be causing you adverse health effects down the road.
Rovner: Yeah, I mean, this is obviously not the first story we’ve seen on this, but it’s certainly one of the most detailed stories that we have seen about this. Well, my story this week is from The Atlantic, by Ron Brownstein. It’s called “Virginia Could Determine the Future of the GOP’s Abortion Policy.” I think he’s right. Virginia votes in odd-numbered years, remember. While Republican Gov. Glenn Youngkin isn’t on the ballot next month, the entire state legislature, which has teetered between Republican and Democratic control over the past several elections, is facing the voters.
Democrats in Virginia, as elsewhere, are charging that if Republicans take back the majority in the State House and Senate, they will restrict abortion, which is likely true, but Republicans say they won’t, quote, “ban abortion,” per se, but would rather set a limit of 15 weeks, with exceptions for rape, incest, and the life of the pregnant person. If voters in a purple state like Virginia see that as a compromise position, rather than a ban, it could set the stage for Republicans elsewhere to fight the current Democratic advantage on the abortion issue. We will see, in about a month, how that all shakes out.
OK, that is our show for this week. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review. That helps other people find us, too. Special thanks, as always, to our amazing engineer, Francis Ying. Also, as always, you can email us your comments or questions. We’re at whatthehealth@kff.org, or you can still find me at X @jrovner or @julierovner at Bluesky and Threads. Sarah?
Karlin-Smith: I’m @SarahKarlin or @sarahkarlin-smith.
Rovner: Lauren.
Weber: I’m @LaurenWeberHP, for health policy.
Rovner: Victoria.
Knight: I’m @victoriaregisk [on X and Threads].
Rovner: We will be back in your feed next week. Until then, be healthy.
Credits
Francis Ying
Audio producer
Emmarie Huetteman
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
2 years 3 weeks ago
COVID-19, Health Industry, Medicaid, Multimedia, Pharmaceuticals, Drug Costs, KFF Health News' 'What The Health?', Podcasts, Prescription Drugs, U.S. Congress, vaccines
PAHO/WHO | Pan American Health Organization
Young people from Brazil, Chile, Colombia, Cuba, Peru, and Mexico win the PAHO Youth Voices 2023 Contest
Young people from Brazil, Chile, Colombia, Cuba, Peru, and Mexico win the PAHO Youth Voices 2023 Contest
Cristina Mitchell
12 Oct 2023
Young people from Brazil, Chile, Colombia, Cuba, Peru, and Mexico win the PAHO Youth Voices 2023 Contest
Cristina Mitchell
12 Oct 2023
2 years 3 weeks ago
Health crisis in Grenada: A call to action for government
“Our nation’s health is not a playing field for political negligence; it is a matter of national urgency that warrants serious and immediate attention”
View the full post Health crisis in Grenada: A call to action for government on NOW Grenada.
“Our nation’s health is not a playing field for political negligence; it is a matter of national urgency that warrants serious and immediate attention”
View the full post Health crisis in Grenada: A call to action for government on NOW Grenada.
2 years 3 weeks ago
Health, PRESS RELEASE, Crime, keith mitchell, new national party, nnp
I'm a psychologist, here's why dreaming about your hobby might be a sign you've become obsessed
The warning signs that you have crossed over into obsessive behavior aren't always obvious, said Singapore psychologist and leadership coach Dr Perpetua Neo, speaking to DailyMail.com.
The warning signs that you have crossed over into obsessive behavior aren't always obvious, said Singapore psychologist and leadership coach Dr Perpetua Neo, speaking to DailyMail.com.
2 years 3 weeks ago