Health Archives - Barbados Today
Barbados lift CARIFTA title
Barbados has again proven itself to have the best triathletes in the region.
For the second year running, Barbados emerged as champions at the CARIFTA Triathlon, Aquathlon and Mixed Relay Championships, which climaxed over the weekend in the Bahamas.
The team captured 15 medals, including an impressive eight gold medals, to amass 180 points and lift the title. The Bahamas was a distant second on 130 points.
Barbados is scheduled to host the 2024 Championships and will be going after a three-peat on home soil. (RB/PR)
The post Barbados lift CARIFTA title appeared first on Barbados Today.
2 years 2 months ago
A Slider, Health, Sports


Here are the 10 drugs that will be up first for Medicare price negotiation
WASHINGTON — Medicare on Tuesday announced it will negotiate prices for 10 drugs, including major blood thinners and diabetes medications, in the first round of its negotiation program created in Democrats’ drug pricing reform law.
The drugs include Bristol Myers Squibb’s blood thinner Eliquis, Boehringer Ingelheim and Eli Lilly’s diabetes drug Jardiance, Johnson & Johnson’s blood thinner Xarelto, Merck’s diabetes drug Januvia, AstraZeneca’s diabetes drug Farxiga, Novartis’ heart failure treatment Entresto, Amgen’s rheumatoid arthritis drug Enbrel, Johnson & Johnson and AbbVie’s blood cancer treatment Imbruvica, J&J’s anti-inflammatory medicine Stelara, and Novo Nordisk insulins that go by names including Fiasp and NovoLog.
2 years 2 months ago
Biotech, Politics, CMS, drug prices, health care policy, Joe Biden, Medicare, White House
Epidemic: Speedboat Epidemiology
Shahidul Haq Khan, a Bangladeshi health worker, and Tim Miner, an American with the World Health Organization, worked together on a smallpox eradication team in Bangladesh in the early 1970s. The team was based on a hospital ship and traveled by speedboat to track down cases of smallpox from Barishal to Faridpur to Patuakhali.
Every person who agreed to get the smallpox vaccination was a potential outbreak averted, so the team was determined to vaccinate as many people as possible.
The duo leaned on each other, sometimes literally, as they traversed the country’s rugged and watery geography. Khan, whom Miner sometimes referred to as “little brother,” used his local knowledge to help the team navigate both the cultural and physical landscape. When crossing rickety bamboo bridges, he would hold Miner’s hand and help him across. “We didn’t let him fall,” chuckled Khan.
Episode 4 of “Eradicating Smallpox” explores what it took to bring care directly to people where they were.
To conclude the episode, host Céline Gounder speaks with public health advocate Joe Osmundson about his work to help coordinate a culturally appropriate response to mpox in New York City during the summer of 2022. “The model that we’re trying to build is a mobile unit that delivers all sorts of sexual and primary health care opportunities. They’re opportunities!” exclaimed Osmundson.
The Host:
Céline Gounder
Senior fellow & editor-at-large for public health, KFF Health News
Céline is senior fellow and editor-at-large for public health with KFF Health News. She is an infectious diseases physician and epidemiologist. She was an assistant commissioner of health in New York City. Between 1998 and 2012, she studied tuberculosis and HIV in South Africa, Lesotho, Malawi, Ethiopia, and Brazil. Gounder also served on the Biden-Harris Transition COVID-19 Advisory Board.
In Conversation with Céline Gounder:
Joe Osmundson
Public health advocate and clinical assistant professor of biology at New York University
Voices from the Episode:
Tim Miner
Former World Health Organization smallpox eradication program worker in Bangladesh
Shahidul Haq Khan
Former World Health Organization smallpox eradication program worker in Bangladesh
Click to open the transcript
Transcript: Speedboat Epidemiology
Podcast Transcript
Epidemic: “Eradicating Smallpox”
Season 2, Episode 4: Speedboat Epidemiology
Air date: Aug. 29, 2023
Editor’s note: If you are able, we encourage you to listen to the audio of “Epidemic,” which includes emotion and emphasis not found in the transcript. This transcript, generated using transcription software, has been edited for style and clarity. Please use the transcript as a tool but check the corresponding audio before quoting the podcast.
TRANSCRIPT
Céline Gounder: In the early 1970s, smallpox was still stalking parts of South Asia. India had launched its eradication program more than a decade before, but public health workers couldn’t keep up with the virus.
Enter … the bifurcated needle.
[Metallic ding sound]
[Light instrumental music begins playing]
Tim Miner: It was a marvelous invention in its simplicity. It looks like a little cocktail fork.
Céline Gounder: You dip the prongs into a bit of vaccine …
Tim Miner: And you would just prick the skin about 12 or 15 times until there was a little trace of blood and then you’d take another one.
Céline Gounder: It barely took 30 seconds to vaccinate someone.
And it didn’t hurt.
Yogesh Parashar: No.
Céline Gounder: Well … it didn’t hurt too much.
Yogesh Parashar: It was just like a pinprick, rapidly done on your forearm. You had a huge supply with you and you just went about and — dot, dot, dot — vaccinated people, carry hundreds with you at one go.
Tim Miner: And you could train somebody in a matter of minutes to do it.
Céline Gounder: Easy to use. Easy to clean. And a big improvement over the twisting teeth of the vaccine instrument health workers had to use before.
The bifurcated needle was maybe 2 and a half, 3 inches long.
Small, but sturdy enough for rough-and-tumble fieldwork.
Yogesh Parashar: It was made of steel. And it used to come in something that looked like a brick. It was just like one of those gold bricks that you see in the movies.
Céline Gounder: And maybe worth its weight in gold.
[Light instrumental music fades to silence]
Céline Gounder: That “cocktail fork” was among the pioneering innovations that helped public health workers wipe out a centuries-old virus.
Tim Miner: You had the bifurcated needle, you had the sterile water, and you had the freeze-dried vaccine, and you could mix them up and off you’d go.
Céline Gounder: Ah, but getting there wasn’t always that easy.
I’m Dr. Céline Gounder, and this is “Epidemic.”
[Epidemic theme music plays]
Céline Gounder: On this episode, we’re exploring what it took to deliver the smallpox vaccine to the people — and all the remaining places — that needed it most.
In South Asia, Bangladesh was a major battleground in the campaign to stop smallpox.
We spoke with a man who helped lead an eradication team there.
Shahidul Haq Khan: My name is MD Shahidul Haq Khan.
Céline Gounder: For our interview, Shahidul Haq Khan invited me to his home in Barishal. That’s in south-central Bangladesh. We sat at a table in the courtyard, and his granddaughter, Kashfia, who looked like she was around 10 years old, stood close by …
Céline Gounder: Kashfia. So nice to meet you, Kashfia. I’m Céline.
Kashfia: Hello.
Céline Gounder: Hello. [Céline chuckles.] Are you going to listen to us?
Céline Gounder: Kashfia wanted to hear her granddad’s stories, and I got the impression that was also important to Shahidul.
As the two of us did our best to communicate through a translator — with neighbors, chickens, and street noise all around — Shahidul wanted me to understand why he was speaking with me and the significance of the smallpox campaign.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: The purpose of saying these things is that we needed all this effort. We put a lot of hard work and effort behind smallpox eradication.
Céline Gounder: Very hard work. You must be very proud of what you helped accomplish.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: Yes, of course. Of course, I can say that we’re proud to say that we’ve eliminated smallpox from this country.
Céline Gounder: The job was to hunt down smallpox — and stop it — in a country packed with people, crisscrossed by rivers, edged with mangrove forests, and dotted with remote lowland river islands.
[Rain sounds fade in]
Céline Gounder: And there were the monsoons. It rained A LOT.
[Bouncy, upbeat music begins playing softly in the background]
[Rain sounds fades out]
Tim Miner: Uh, well, we got wet. [Tim chuckles.] To state the obvious.
Céline Gounder: That’s Tim Miner. He was an officer with the World Health Organization in Bangladesh.
Tim Miner: My legal name is Howard Miner, but I was the third Howard, so I got nicknamed Tim.
Céline Gounder: Shahidul and Tim worked together for several months in 1974.
The public health strategy was called “search and containment,” and a big part of that meant figuring out how to get the vaccine from one community to the next.
Tim Miner: And occasionally you have to park your motorcycle, take your shoes and socks off, and walk across a leech-infested paddy field to get to the next case.
Céline Gounder: The work depended on local knowledge, and Shahidul was the local knowledge.
He was the lead Bangladeshi member on the eradication team, and when they arrived at a village that had a suspected case of smallpox, often Shahidul went in first, with Tim a few steps behind …
Tim Miner: Someone would bring out some chairs. And sometimes we would have tea and biscuits. Or, if they didn’t have tea and biscuits, then somebody would climb up and get a coconut and chop off the top and watch me drink it and dribble the coconut milk all over myself, and everybody had a good time.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: Dr. Miner called me “little brother.” I was younger then. How old was I? 21 or 22 years old.
Tim Miner: He referred to me as “Dr. Miner,” even though I’m not a … a physician. That’s how he referred to me.
Céline Gounder: Shahidul had been working in public health before he joined the smallpox effort. He offered guidance on culture — and occasionally gave Tim a hand on rickety bamboo bridges.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: Most of the time, I escorted him across the bamboo bridge. I took his bag and held his hand and helped him across.
Tim Miner: You learn to walk and not look down and just, uh, you know, hang onto the poles. And, fortunately, I never fell in.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: We didn’t let him fall.
[Bouncy, upbeat music fades out]
Céline Gounder: The team was based on a hospital ship, called the Niramoy. It had all the basics: a couple of cabins, a space to perform surgery, plus a few comforts, like a generator they’d turn on in the morning for showers, a cook who picked up fresh fish at the market every day.
Tim Miner: I would have a doodh cha, a tea with milk, and a kacha morich pyaz — scrambled eggs with, uh, chiles.
Céline Gounder: The hospital ship hauled supplies from port to port. And everywhere they went, they towed a speedboat along with them.
Tim Miner: We would receive reports of cases and we would get down from the ship in our speedboat, and the speedboat driver would take us as far as the boat could go. And we would walk, do the investigation, and find out who the contacts were and vaccinate the village and surrounding areas.
Céline Gounder: Tim calls it “speedboat epidemiology.” The work required a willingness to go wherever and everywhere the virus took up residence. By and large, people welcomed them and were glad to get the vaccine.
Tim Miner: They know about smallpox. They’ve been dealing with it, you know, all of their lives. And they have lost family members to the disease.
Céline Gounder: Still, the task was huge: to find and vaccinate every person with smallpox — and all the people that person had come in contact with.
[Subtle music begins playing]
Céline Gounder: In modern-day public health, the work gets done with cellphones and spreadsheets, maybe social media. In Bangladesh in 1974, they had none of that.
Shahidul and Tim had the speedboat, motorbikes, and their feet to cover a territory that took them all the way down to the coast.
Tim Miner: First there’s Barishal …
Shahidul Haq Khan: Latachapli …
Tim Miner: … then there’s Faridpur …
Shahidul Haq Khan: … Dankupara …
Tim Miner: … then there’s Patuakhali.
Shahidul Haq Khan: … and Kuakata.
Céline Gounder: People were constantly on the move — maybe for seasonal work or better opportunities. That made contact tracing tricky. During one investigation, Tim identified a man who’d been exposed to the virus, but he’d left the region for Dhaka.
The capital was densely populated — a city of 2 million in 1974. And smallpox was highly contagious. So Tim called a colleague — on the shortwave radio — to see if he could track down the man in Dhaka.
[Ambient Dhaka street noises play in the background]
Tim Miner: Well, it’s not just a street address or a ZIP code or anything like that, as you can well imagine. He lived in a basti, or a slum. And I described it as best I could. You know, ‘You enter by the big tree and turn left at the tea stall and walk the path and then start calling out for the family name.’
Céline Gounder: They found the guy! And vaccinated him. Tim says the man had smallpox, but the virus hadn’t quite erupted yet, so it was a pretty mild case.
Tim Miner: Because of his immunization. It is somewhat miraculous, the needle in the haystack.
[Music fades out]
Céline Gounder: In Bangladesh, people weren’t likely to just show up to a local clinic to get the vaccine, so the team took the vaccine to the people.
At its best, public health follows and bends to the rhythm of the culture. For example, after Ramadan, as Muslims began to break the fast for Eid …
Tim Miner: Where people go back to their villages and visit and bring presents and gifts and food.
[Ambient sounds of the water from a port in Bangladesh play]
Céline Gounder: The team went to ports where steamer ships departed, asking in Bengali if travelers had come in contact with anyone with the disease’s distinctive pustules.
Tim Miner: Guṭibasanta, uh, basanta rōgī.
Céline Gounder: Which means “smallpox patient.”
Tim Miner: Have you seen any guṭibasanta and basanta rōgī?
Céline Gounder: Tim says he relied on his team to figure out how best to make the person in front of them comfortable.
Tim Miner: ‘What would you do? What do you think should be done in this case?’ And I don’t think this is done often enough. It was a real partnership. It was real working together.
Céline Gounder: Well, a partnership, yes. But Shahidul Haq Khan says the search-and-containment program was pretty strict. His work was meticulously checked and checked again.
Remember, he was maybe 21 or 22 years old, with a big responsibility on his shoulders, and Tim Miner was a tough boss.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: At any cost, we had to vaccinate all. There was no other way.
Céline Gounder: Sometimes Shahidul had to return to the same home over and over — or hang out, if the man of the house was still in the fields working.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: We had to wait until they returned.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: Otherwise, Dr. Miner would again take us back there, no matter how late. [Shahidul laughs]
Céline Gounder: One evening, Shahidul returned to the hospital ship after a day of door-to-door canvassing, and had to give a not-so-great report to Tim.
[Tense music begins playing]
Shahidul Haq Khan: [Shahidul speaking in Bengali] … a pregnant, uh, …
English translation: I couldn’t vaccinate a pregnant woman in Dankupara. This was the first time that I couldn’t vaccinate someone.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: I couldn’t convince her at all. He immediately told us to pack up. He stopped the work and said, “Let’s go.”
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: Immediately. At that very moment.
Tim Miner: We were working basically 24/7, if need be.
Céline Gounder: The team headed to the speedboat. It was late. And it was freezing. Shahidul remembers the bite of the cold air as they blasted across the water toward the woman’s village.
Tim Miner: I fully understand, understood why this woman hesitated to be vaccinated. She was expecting a child and she didn’t want to do anything to jeopardize her life or the life of the unborn child. So, we were very gentle in talking with her and answering her questions. It was time well spent.
Céline Gounder: The woman agreed to take the vaccine.
Shahidul Haq Khan: [Shahidul speaking in Bengali]
English translation: That day was one of the most memorable of my life.
[Music fades to silence]
Céline Gounder: Many on the team considered their outreach to women fundamental to success in South Asia, because … women talk.
What they say, what they believe, echoes.
Tim Miner: They get together, they do the laundry, they do the cooking, they share good times and bad times. This woman who was vaccinated probably showed her vaccination either in her family or in the village. And that’s the importance of getting one person, especially a pregnant woman who will tell others about immunization.
Céline Gounder: Public health workers trying to end smallpox across South Asia mostly had the same tools — the vaccine, that bifurcated needle, and a strategy — on paper. But squashing the virus required tactics specific to each community: its needs, its culture, its worries … and its terrain.
[Staccato music begins playing]
Céline Gounder: Smallpox eradication workers went to great lengths to meet people where they were.
But Joe Osmundson, who’s a public health advocate in New York City, told me that’s not an approach we see nearly enough in public health today.
Joe Osmundson: Céline, it’s not your first time at the rodeo. [Celine laughs] Um, it’s like, we’ve all been through this again and again and again.
We know what the problems are and yet we seem reluctant to actually do the right thing, which is to build processes that meet people where they’re at.
Céline Gounder: After the break, more on what it looks like to bring public health directly to those who need it most.
[Music fades to silence]
Céline Gounder: Mpox, formerly known as monkeypox, is a highly contagious virus. Last summer, mpox cases spiked around the world, spreading quickly, predominantly among men who have sex with men. Mpox spreads through physical contact. It causes a painful blistering rash and, in extreme cases, it can be deadly.
My colleague Joe Osmundson acted as a community liaison for the New York City Department of Health to help coordinate a culturally appropriate response to mpox.
Joe Osmundson: I’m a microbiologist by training, but I also just do tons of advocacy and activism as a queer person who believes in equal access to the best biomedicine available.
Céline Gounder: As mpox cases were increasing, we knew we needed to vaccinate those at highest risk as quickly as possible. Joe’s plan? Mobile vans to quickly bring mpox vaccines to places where high-risk people already were.
Joe Osmundson: Our idea was to go to commercial sex venues, because commercial sex venues self-select for people with a large number of sexual partners. And if you give them the best possible immunity, that protects not just the people at the party but all the other people in the larger sexual network that they connect with.
Céline Gounder: What is a commercial sex venue?
Joe Osmundson: It’s basically a nonhousehold space where people gather for sex.
When you have public venues where people gather, you have the opportunity to meet them where they’re at, to provide education, to provide condoms, to provide access to HIV testing and access to health care.
So many queer people don’t have affirming doctors, don’t feel comfortable asking about sexual health with their physicians. So, you can put a van outside with affirming physicians and actually provide that preventative care that actually stops the infection.
Céline Gounder: Did you run into any obstacles in doing this outreach? Setting up the mobile vans …?
Joe Osmundson: So, there is a huge amount of mistrust in this community for city officials, for good reason. For many decades there was a group inside the New York City Department of Health that had undercover people who would go to these parties and find violations and close them down. So really it was only me and a couple other people doing outreach on-site.
Céline Gounder: How did it work, what was the scene like, and what was your role in that?
Joe Osmundson: Yeah, so, when I was there, I would go inside the club and, you know, there’s a little line, an area where people get dressed or undressed, and I would just hang out there and people would have a lot of questions.
So, because, again, they perceived me as being, like, a part of their community, it was very easy to talk to people and just ask, you know, “Hey, have you had your vaccine yet? Have you had both doses?” If not, you know, it’ll take 15 minutes. I can walk you down to the van and get you that dose tonight.
Céline Gounder: Were these mobile vaccination vans successful?
Joe Osmundson: We find them to be massively successful. Once the city was able to get the vans there, people were so grateful to be able to get a shot on-site.
We were giving 60, 80 doses per event — when the event might only have 140 people — so we were vaccinating 60% of these parties.
That’s the other magic of the mobile units, was that you had people queer people talking to queer people, and even queer people of color talking to queer people of color and offering the care in terms that that community knows how to respond to and also just has more inherent trust with.
Céline Gounder: But, at the same time, in New York City, mpox vaccination rates have been disproportionately low in Black communities.
Joe Osmundson: Mm-hmm.
Céline Gounder: As well as Hispanic communities.
What could public health leaders have done from the start to ensure more equitable vaccine distribution, and what should they be doing now?
Joe Osmundson: Yeah. It was a remarkable sort of mistake that, not just New York, but many cities made where they said we’ll build the foundation and then worry about equity later, because this is an emergency.
So we’ll open up a brick-and-mortar in Chelsea, and then we’ll get the vaccine vans up at, you know, Brooklyn Pride, a Bronx health clinic. You know, we’ll do that later.
We know that if you don’t do equity as the foundation, you will be chasing disparities.
Céline Gounder: What can we say about who’s been vaccinated and who remains unvaccinated?
Joe Osmundson: Black people are undervaccinated. They also have a higher rate of advanced HIV infection, and mpox plus advanced HIV means really severe disease and even death. Ninety percent of mpox deaths have been in Black people, Black queer people with advanced HIV.
And we need something brand-new because we’ve been failing these folks for years. They have so many horrific experiences with their health care providers, or they don’t have insurance, or they’re underemployed, or they live super far from the nearest health care clinic.
When people have difficulties accessing care, it spreads to every disease state, from HIV to mpox to primary care, etc.
Céline Gounder: How can we apply this model of health outreach beyond mpox?
Joe Osmundson: The model that we’re trying to build is a mobile unit that delivers all sorts of sexual and primary health care opportunities. They are opportunities! You know? If someone’s getting a covid vaccine, give them a flu vaccine at the same time. The literature shows that these interventions work.
Céline Gounder: What else is there beyond vans? Are there other strategies when it comes to reaching people where they are that we haven’t employed that we should be thinking about?
Joe Osmundson: We have affirming clinicians, affirming Black queer clinicians all over this city. Their expertise should be fostered.
For years there’s been this model of health officials talking to community. And that’s outreach. And we aren’t done with that.
We have experts, we have clinicians, we have epidemiologists, we have scientists who are in the community who know the science just as well as health officials. And communication needs to go two ways.
Céline Gounder: That was Joe Osmundson, a microbiologist at New York University and the author of the book “Virology.”
Joe Osmundson: The sexiest public health outreach worker of all time! [Laughter] A face made for radio. [Laughter]
[“Epidemic” theme music begins playing]
Céline Gounder: Next time on “Epidemic” …
Larry Brilliant: Your company is sending death all over the world. You’re the greatest exporter of smallpox in history … You’ve got to stop this.
Céline Gounder: “Eradicating Smallpox,” our latest season of “Epidemic,” is a co-production of KFF Health News and Just Human Productions.
Additional support provided by the Sloan Foundation.
This episode was produced by Taylor Cook, Zach Dyer, and me.
Redwan Ahmed was our translator and local reporting partner in Bangladesh.
Managing editor Taunya English was scriptwriter for the episode — with help from Stephanie O’Neill.
Oona Tempest is our graphics and photo editor.
The show was engineered by Justin Gerrish.
Voice acting by Pinaki Kar.
We had extra editing help from Simone Popperl.
Music in this episode is from the Blue Dot Sessions and Soundstripe.
We’re powered and distributed by Simplecast.
If you enjoyed the show, please tell a friend. And leave us a review on Apple Podcasts. It helps more people find the show.
Follow KFF Health News on Twitter, Instagram, and TikTok.
And find me on Twitter @celinegounder. On our socials, there’s more about the ideas we’re exploring on the podcasts. And subscribe to our newsletters at kffhealthnews.org so you’ll never miss what’s new and important in American health care, health policy, and public health news.
I’m Dr. Céline Gounder. Thanks for listening to “Epidemic.”
[“Epidemic” theme fades out]
Credits
Taunya English
Managing editor
Taunya is senior editor for broadcast innovation with KFF Health News, where she leads enterprise audio projects.
Zach Dyer
Senior producer
Zach is senior producer for audio with KFF Health News, where he supervises all levels of podcast production.
Taylor Cook
Associate producer
Taylor is associate audio producer for Season 2 of Epidemic. She researches, writes, and fact-checks scripts for the podcast.
Oona Tempest
Photo editing, design, logo art
Oona is a digital producer and illustrator with KFF Health News. She researched, sourced, and curated the images for the season.
Additional Newsroom Support
Lydia Zuraw, digital producer Tarena Lofton, audience engagement producer Hannah Norman, visual producer and visual reporter Simone Popperl, broadcast editor Chaseedaw Giles, social media manager Mary Agnes Carey, partnerships editor Damon Darlin, executive editor Terry Byrne, copy chief Gabe Brison-Trezise, deputy copy chiefChris Lee, senior communications officer
Additional Reporting Support
Swagata Yadavar, translator and local reporting partner in IndiaRedwan Ahmed, translator and local reporting partner in Bangladesh
Epidemic is a co-production of KFF Health News and Just Human Productions.
To hear other KFF Health News podcasts, click here. Subscribe to Epidemic on Apple Podcasts, Spotify, Google, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
2 years 2 months ago
Multimedia, Public Health, Epidemic, Podcasts, vaccines
Leptospirosis has caused 23 deaths In the Dominican Republic
Santo Domingo.- With the recent passing of tropical storm Franklin causing floods, the first seven months of this year have seen a worrying surge in leptospirosis cases in the country. Leptospirosis is a disease transmitted through contact with contaminated animal urine. The floodwaters left behind by the storm provide an environment conducive to its spread.
Santo Domingo.- With the recent passing of tropical storm Franklin causing floods, the first seven months of this year have seen a worrying surge in leptospirosis cases in the country. Leptospirosis is a disease transmitted through contact with contaminated animal urine. The floodwaters left behind by the storm provide an environment conducive to its spread.
As of the fifth of this month, the nation has reported 23 deaths and 259 cases of leptospirosis. This figure is a staggering 89% higher than the numbers recorded up to the same date last year, when there were 136 infections and 21 deaths.
The latest epidemiological report for week 31 shows that thirteen suspected cases of leptospirosis emerged during that week. These cases were identified in various provinces, including San Cristóbal, San Juan de la Maguana, Santiago de los Caballeros, Santo Domingo, La Vega, Puerto Plata, Sánchez Ramírez, and the National District.
Eladio Pérez, Vice Minister of Collective Health, had earlier issued an epidemiological alert, aiming to ensure that Provincial Directorates and Health Areas are equipped to respond to health situations as they arise.
2 years 2 months ago
Health
Medical News, Health News Latest, Medical News Today - Medical Dialogues |
ESC 2023 Update: Patients urged to be vigilant about cardiac infections
Patients with specific cardiac conditions such as valvular heart disease and congenital abnormalities, or those requiring a pacemaker, should practice good dental and skin hygiene to help prevent rare but potentially deadly infections of the heart’s inner lining and valves, according to European Society of Cardiology (ESC) Guidelines on infective endocarditis, published online to
day in European Heart Journal.
“Infective endocarditis is an uncommon but very serious disease that can present with many different symptoms, and thus may be challenging to diagnose,” said Guidelines task force chairperson Professor Michael Borger of Leipzig Heart Centre, Germany. “Patient education is therefore paramount to early diagnosis and treatment. Those with valvular heart disease or previous heart valve surgery should be particularly diligent with regards to prevention and recognising symptoms.”
Infective endocarditis refers to an infection of the heart’s inner lining, most frequently the heart valves. It occurs when bacteria or fungi enter the bloodstream, for example through skin infections, dental procedures and surgery. Symptoms include fever, night sweats, unexplained weight loss, cough, dizziness and fainting. The infection can lead to destruction of the valve, abscesses and clusters of microbes and cells, which can break into smaller parts that travel to other areas of the body (called embolisation). Heart failure, septic shock and stroke can also occur.
Worldwide each year there are nearly 14 new cases of infective endocarditis for every 100,000 individuals and more than 66,000 patients die. “The mortality rate is extremely high and therefore preventive strategies in patients at high risk are pivotal,” said Guidelines task force chairperson Dr. Victoria Delgado of the Germans Trias i Pujol University Hospital, Badalona, Spain.
Those at highest risk include survivors of previous episodes of infective endocarditis and patients with prosthetic heart valves, congenital heart disease (not including isolated congenital heart valve abnormalities) or a left ventricular assist device. In these patients, prophylactic antibiotics are recommended before oral or dental procedures. Patients at intermediate risk are those with pacemakers, severe valvular heart disease, congenital heart valve abnormalities (including bicuspid aortic valve) and hypertrophic cardiomyopathy, a disease where the heart muscle is thickened. In these patients, the need for antibiotic prophylaxis prior to dental procedures should be evaluated on an individual basis. Antibiotic prophylaxis is not needed in those at low risk.
The main targets for antibiotic prophylaxis are oral streptococci. The document states that “the emerging and increasing antibiotic resistance among oral streptococci is of concern”. Dr. Delgado said: “Streptococci are naturally present in the mouth but can enter the bloodstream when oral hygiene is suboptimal and during dental procedures. Rises in antibiotic use for infectious diseases have led to resistance, meaning that antibiotics become ineffective. Caution in the use of antibiotics is therefore needed and self-medication should be avoided.”
The Guidelines recommend other preventive measures for patients at intermediate and high risk including twice daily tooth cleaning, professional dental cleaning (twice yearly for high risk and yearly for intermediate risk patients), consulting a general practitioner for fever with no obvious
reason, strict skin hygiene, treatment of chronic skin conditions, and disinfection of wounds. Piercings and tattoos are discouraged.
Recommendations are provided for diagnosis, treatment, and management of complications. Diagnosis is based on clinical suspicion, blood cultures, and imaging. Echocardiography is the first line imaging technique, and new diagnostic criteria include findings on other imaging techniques. There are new recommendations on the use of computed tomography, nuclear imaging and magnetic resonance imaging plus novel diagnostic algorithms when the infection involves native heart valves, prosthetic heart valves, and implanted cardiac devices such as pacemakers and defibrillators.
Treatment aims to cure the infection and preserve heart valve function. The Guidelines recommend appropriate antibiotics, determined from blood cultures, as the mainstay of therapy, with duration depending on the severity of infection. Surgery to remove infected material and drain abscesses is indicated for patients with heart failure or uncontrolled infection, and to prevent embolisation. Surgery should generally occur earlier than previously recommended because of improved survival.
One of the worst complications of endocarditis is stroke. Decisions about the timing of surgery in patients who have suffered a stroke must balance the risk of neurological deterioration during the procedure against that of delaying surgical therapy. Novel recommendations are to proceed with urgent heart valve surgery in patients with ischaemic stroke due to embolism but delay surgery in patients with haemorrhagic stroke. In addition, thrombectomy (removal of the embolus through a catheter) may be considered in very select patients with stroke.
A new section in the Guidelines is devoted to patient-centred care and shared decision-making. Professor Borger said: “Infective endocarditis is a life-threatening condition with lengthy treatment and can be emotionally distressing for patients and families. Patients must be at the centre of care to achieve the best physical and mental outcomes.”
2 years 2 months ago
Cardiology-CTVS,Cardiology & CTVS Guidelines,Top Medical News,Latest Medical News

The Journey to Personalized Healthcare
The Walt Disney Company excels in designing exceptional service because they are hyper-focused on listening, tracking, designing, and measuring the experiences of guests visiting their properties. We can apply this approach in pharma by enhancing our patient journey maps and go beyond focusing on the key clinical engagement touch points (e.g., doctor visits, prescription pickups) and enriching our insights with the micro-moments surrounding these obvious events.
2 years 2 months ago
BioPharma, Daily, MedCity Influencers, Top Story, biopharma nl, Patient Engagement
Health Archives - Barbados Today
Suriname bans the sale of electronic cigarettes
(CMC) – Suriname has been named among eight countries that are adopting measures in line with the World Health Organization’s (WHO) Framework Convention on Tobacco Control (FCTC) to protect the health of their populations from novel tobacco products.
The WHO said Friday that with the recent ban on the use and marketing of electronic cigarettes in Venezuela, currently, 21 countries in the Americas regulate electronic nicotine delivery systems (ENDS), such as e-cigarettes and vapes.
“The resolution that regulates new and emerging nicotine and tobacco products in Venezuela is an important step forward for the country and for the region,” said Dr Anselm Hennis, Director of Non-Communicable Diseases Mental Health at the Pan American Health Organization (PAHO/WHO).
“We hope that this measure motivates other countries to take action on these products, which are addictive, harmful and aggressively advertised towards the youngest,” he added.
The eight new countries to join the initiative are Argentina, Brazil, Mexico, Nicaragua, Panama, Suriname, Uruguay and Venezuela and PAHO said these countries prohibit their sale altogether, and the other 13 countries have partially or totally adopted one or more regulatory measures.
It said 14 countries in the Americas, including the Caribbean, lack any regulation of these products.
Last June, a previous resolution of the Venezuelan Ministry of Popular Power for Health banned the sale of vapes to minors.
Now, the August 1 resolution prohibits “the manufacture, storage, distribution, circulation, commercialization, importation, exportation, use, consumption, advertising, promotion and sponsorship of ENDS and electronic non-nicotine delivery systems (ENNDS)”, as well as their “consumables”, “accessories”, and “heated tobacco products”.
PAHO said e-cigarettes are the most common form of electronic nicotine delivery systems. When used, they heat a liquid to create aerosols that are inhaled by the user.
It said these “e-liquids” contain nicotine, a highly addictive substance found in tobacco, and other additives, flavorings and chemicals, some of which are toxic to the health of both the user and those exposed to them.
PAHO/WHO recommends that governments implement regulations in line with the provisions of the FCTC and its decisions, such as prohibiting the marketing of ENDS, including their importation, distribution or sale, as well as regulations on their use in public places, prohibiting their advertising and promotion, taxing them, and other regulations similar to those applied to tobacco products.
Tobacco kills one million people in the region of the Americas annually and while measures taken since the FCTC came into force in 2005 ha per cent in 2020, these achievements are threatened by novel tobacco and nicotine products.
Currently, 11.3 per cent of adolescents between 13 and 15 years of age in the region use tobacco, compared to the world average of 10.3 per cent.
The post Suriname bans the sale of electronic cigarettes appeared first on Barbados Today.
2 years 2 months ago
A Slider, Health, Local News

Benefits of digitalization highlighted for medical tourism in the Dominican Republic
The Dominican Republic’s healthcare sector has been working “hard” on digitalization; since the pandemic, efforts have increased.
The significant changes impacting the global healthcare system have led its main actors to adopt more modern, interconnected, and patient-centered digital systems.
The Dominican Republic’s healthcare sector has been working “hard” on digitalization; since the pandemic, efforts have increased.
The significant changes impacting the global healthcare system have led its main actors to adopt more modern, interconnected, and patient-centered digital systems.
Therefore, Fedor Vidal, CEO of Arium Salud Digital, maintains that one of the objectives of the digitalization of healthcare is artificial intelligence, which has produced excellent results.
He indicated that “about health tourism, we see great benefits regarding the identification of procedures and services in which the country could be a leader in the region; the comparative analysis of attention costs and quality indexes compared with other countries.”
He stressed that this is only possible with digitalizing clinical processes and adherence to international clinical coding protocols.
“Another benefit of artificial intelligence being used in the health tourism sector is the identification of potential patients within the general population of tourists through population profiles and aggregated data,” he explained.
Axes of impact
The healthcare industry has been positively marked in four axes thanks to digital transformation, which are: Exponential increase in the efficiency of administrative processes, access to quality healthcare to more people, more quickly and more safely, democratization of information for all actors in the sector and the interconnection of actors in a synergistic way through fluid electronic processes allowing the flow of information between them in an expeditious manner.
Vidal said that one of the main steps to be taken is to educate oneself on the subject of hospital digital transformation through congresses and seminars that are held annually, such as the International Congress on Health and Wellness Tourism.
2 years 2 months ago
Health, tourism
Avoid those pesky germs
SUMMER is almost over. Summer camps are done, children are returning home from vacation at grandma's or cousin's house — free paper bun, and it's time to get ready for back-to-school!
Whether your child is about to start a new school or a new grade, it's important to instil healthy habits. In the words of my very good friend, "Germs still keeping".
SUMMER is almost over. Summer camps are done, children are returning home from vacation at grandma's or cousin's house — free paper bun, and it's time to get ready for back-to-school!
Whether your child is about to start a new school or a new grade, it's important to instil healthy habits. In the words of my very good friend, "Germs still keeping".
Germs are everywhere. There are germs on every single surface we come in contact with, including our skin. And yes, the COVID-19 virus is still going around. If we teach our children about germs and how we can prevent the spread of germs, we can avoid many infections and trips to the doctor and hospital.
Here are some tips for you and your child as they head back-to-school.
*Get a check-up before school to identify any potential health concerns early
*If your child has a chronic illness like asthma, sickle cell or a heart condition, make sure you have all the necessary medications he/she needs
*Inform your child's (new) teacher about any health conditions and how to manage them; for example, what to do in situation like an asthma attack or seizure
*If your child needs to carry medications to school (for example, asthma pumps), teach them where to find the medications in their school bag and how to use them (of course, this is age appropriate).
*Inform the school if your child has any food allergies and teach your child about food allergies, and why they should NOT eat from other students. A peanut butter sandwich from an unknowing schoolmate could be very dangerous to a child with peanut allergies.
*Especially for preschool age group (two to five years), remember it is quite normal for children to get sick every three to four weeks
*Teach and encourage good hand hygiene. Wash hands frequently, use hand sanitisers, and wash hands especially if they are visibly dirty.
*Teach and encourage children how to cough into their elbow and not their hands, how to blow their nose or sneeze into a tissue which should be disposed right away followed by immediate hand washing. If you sneeze or cough into a rag, anything that touches that rag (hands, books, contents of their bag) are contaminated with germs.
*Keep kids out of school if sick especially if the illness is contagious — fever, coughing, runny nose, vomiting or diarrhoea. Think bodily fluids that can disseminate/spread easily
*If your child has a fever, keep out of school until fever-free for at least 24 hours
*Make sure children are up to date with their vaccines. Remember, the COVID vaccine is available for children 12 and older. If your child is immunocompromised (very prone to getting sick easily based on an underlying health condition), consider getting vaccines like the pneumoccal vaccine, chicken pox and rotavirus vaccine. Ask your doctor about these non-government issued vaccines.
*Keep in mind seasonal illnesses like hand foot and mouth disease, chicken pox, running belly. Know what symptoms to look for, and how to prevent these illnesses. Right now, dengue fever is on the rise, so protect your little ones with mosquito repellents at home and school.
*Consider a "worm out". Deworming is safe, easy and inexpensive. "Worm medicine" gets rid of possible parasites in the intestines that may potentially cause serious health issues like anaemia and blockage in the intestines. Deworming is usually done one to two times a year.
In addition, schools usually require a "medical" to be done before the start of a new school year. The school usually provides a medical form for you to carry to your doctor to have completed. If you haven't already done this, here is what to expect.
There may be a section for you, the parent, to fill out — name, address, date of birth, etc. There is also a section to fill out child's immunisations.
Your child's weight, height, vitals and blood pressure will be done. The doctor will examine your child from head to toe, including vision test, hearing evaluation, checking the skin, ears, listening to the chest (heart and lungs) and tummy with a stethoscope and checking all limbs (arms and legs). Some medicals require a urine test to look for blood, sugar and protein. There is also a section to document how much physical activity your child can tolerate (normal, as tolerated or limited).
Based on the information provided and the examination findings, the doctor will establish if your child is well, if he/she needs any further tests to be done (and will write requests for those), write a prescription if needed, or refer your child to see a specialist if they see fit.
Happy back-to-school!
Dr Tal's Tidbits
Before heading back-to-school, make sure your child gets a medical/check up that may pick up any health concerns to ensure a healthy, safe school term.
Dr Taleya Girvan has over a decade's experience treating children at the Bustamante Hospital for Children, working in the Accident and Emergency Department and Paediatric Cardiology Department. Her goal is to use the knowledge she has gained to improve the lives of patients by increasing knowledge about the health-care system in Jamaica. Dr Tal's Tidbits is a series in which she speaks to patients and caregivers, providing practical advice that will improve health care for the general population. E-mail: dr.talstidbits@gmail.com IG @dr.tals_tidbits.
2 years 2 months ago
A comprehensive guide to staying medically safe at large events
In
a few hours, Jamaica is set to witness one of the largest musical events of the summer. The "Under the Influence" concert featuring international recording artist Chris Brown is set to go live at the National Stadium with an estimated crowd pull of nearly 30,000 patrons.
In
a few hours, Jamaica is set to witness one of the largest musical events of the summer. The "Under the Influence" concert featuring international recording artist Chris Brown is set to go live at the National Stadium with an estimated crowd pull of nearly 30,000 patrons.
Large public events, such as this, are exhilarating experiences that bring people together to enjoy music and create lasting memories. However, these events also present certain health and safety challenges, especially considering the potential for overcrowding and exposure to various risks. Ensuring medical safety at such events is paramount to ensuring a positive experience for all attendees.
Heart Institute of the Caribbean (HIC) is a key sponsor of this event and the emergency medical service team of (HIC) has been engaged to provide emergency medical coverage for this event. The HIC EMS team will comprise 42 medical personnel including emergency medicine trained physicians, critical care personnel, nurses, technologists, EMTs and other paramedical and allied health workers to staff six emergency medical stations at the venue ensuring that patrons have easy and ready access to medical personnel for any urgent or emergency medical needs.
We are also supporting the team with two advanced medical ambulances fully equipped with all resuscitative equipment and materials to stabilise individuals prior to transfer to receiving hospitals. Our HIC Heart Hospital will also be on high alert for acute heart-related conditions that may arise during the event. In today's column, we explore essential strategies and precautions to keep medically safe at this event and other public events.
1) Pre-event preparation
Before attending a large public event such as this, it's crucial to engage in some pre-event preparation to set the stage for a safe experience. Familiarise yourself with the layout of the venue, including entrances, exits, medical aid stations, and restrooms. This knowledge can prove invaluable in case of emergencies. Outdoor events are often susceptible to weather changes. It is advisable to check the weather forecast before attending and dress appropriately to stay comfortable and avoid exposure to risk of heatstroke or hypothermia.
2) Stay well-hydrated and have a meal before the event.
Dehydration and low blood sugar can lead to dizziness, fainting, fatigue, and other health problems.
3) Personal health precautions
Taking care of your personal health is essential to staying safe at a large public event. If you have a pre-existing medical condition or chronic illness, it would be helpful to carry a small card with your essential medical information including emergency contacts and listing of your chronic conditions. Such information could prove invaluable in case of an emergency and will be useful to the medical personnel if you require assistance. If you're on medication, make sure to have an adequate supply with you. Consider setting reminders to take them on time. For individuals with allergies, it would pay to be cautious about potential allergens present at the event, such as food, pollen, perfumes, or certain fabrics.
4) Hygiene and sanitation
Maintaining good hygiene practices can help prevent the spread of illnesses. Carry a small bottle of hand sanitiser and use it regularly, especially after touching surfaces like handrails and restroom facilities. This will reduce your risk of exposure to infectious agents, especially viruses. Respiratory etiquette should always be employed. If you're coughing or sneezing, cover your mouth and nose with a tissue or cough in your elbow to prevent the spread of germs to others.
5) Responsible use of alcohol
If you choose to consume alcohol, do so in moderation and avoid unpredictable combinations. Excessive drinking can impair judgement and increase the risk of accidents and injury. Avoid the use of illegal substances, as they can have unpredictable and potentially dangerous effects on your health.
6) Crowd safety
Navigating through large crowds requires some specific safety considerations. While enjoying the event, be mindful of personal space. Proximity to others might increase the risk of transmitting or contracting illnesses. We are learning to live with COVID but be mindful that the epidemic has not disappeared even though we have learned to coexist with it. Large crowds increase risk of transmission and so adequate precaution would be in order. Pay close attention to the flow of the crowd. Sudden surges or changes in direction can lead to accidents and injuries.
7) Locate HIC emergency medical stations
As previously noted, there will be six HIC emergency medical stations on site. It would pay to familiarise yourself with their locations upon arrival. Make a mental note of where the medical stations are located. These stations are staffed with medical personnel and equipped to handle injuries and acute health issues. If you feel unwell or witness someone in distress, don't hesitate to approach event staff or security personnel for assistance.
8) Know emergency exits
Be aware of the nearest emergency exits should you need to evacuate quickly. If there is an urgent need for evacuation, do not panic. Follow instructions from security personnel and organisers and evacuate purposefully to avoid stampede and unnecessary injury. In conclusion, attending large public events like musical concerts can be both thrilling and safe with the right precautions. From pre-event preparation to responsible behaviour during the event, taking these steps can significantly reduce health risks and contribute to a positive experience for everyone involved. Remember, personal safety is a shared responsibility, and by looking out for one another, we can create an environment where everyone can enjoy the event to the fullest while staying medically secure. HIC emergency medical team remains poised to respond quickly in the event of an emergency and committed to ensuring the safety of event attendees.
Dr Ernest Madu, MD, FACC and Dr Paul Edwards, MD, FACC are consultant cardiologists for the Heart Institute of the Caribbean (HIC) and HIC Heart Hospital. HIC is the regional centre of excellence for cardiovascular care in the English-speaking Caribbean and has pioneered a transformation in the way cardiovascular care is delivered in the region. HIC Heart Hospital is registered by the Ministry of Health and Wellness and is the only heart hospital in Jamaica. Send correspondence to info@caribbeanheart.com or call 876-906-2107.
2 years 2 months ago
Eight countries in the Americas ban electronic cigarettes
WASHINGTON, DC (PAHO) - With the recent ban on the use and mar
keting of electronic cigarettes in Venezuela, more countries in the Americas are adopting measures in line with the World Health Organization's (WHO) Framework Convention on Tobacco Control (FCTC) to protect the health of their populations from novel tobacco products.
WASHINGTON, DC (PAHO) - With the recent ban on the use and mar
keting of electronic cigarettes in Venezuela, more countries in the Americas are adopting measures in line with the World Health Organization's (WHO) Framework Convention on Tobacco Control (FCTC) to protect the health of their populations from novel tobacco products.
"The resolution that regulates new and emerging nicotine and tobacco products in Venezuela is an important step forward for the country and for the region," said Dr Anselm Hennis, director of non-communicable diseases mental health at the Pan American Health Organization (PAHO). "We hope that this measure motivates other countries to take action on these products, which are addictive, harmful and aggressively advertised towards the youngest," he added.
Currently, 21 countries in the Americas regulate electronic nicotine delivery systems (ENDS), such as e-cigarettes and vapes, in some way. Eight of them (Argentina, Brazil, Mexico, Nicaragua, Panama, Suriname, Uruguay, and Venezuela) prohibit their sale altogether, and the other 13 have partially or totally adopted one or more regulatory measures. Meanwhile, 14 countries lack any regulation of these products.
Last June, a previous resolution of the Venezuelan Ministry of Popular Power for Health banned the sale of vapes to minors. Now, the August 1 resolution prohibits "the manufacture, storage, distribution, circulation, commercialisation, importation, exportation, use, consumption, advertising, promotion and sponsorship of ENDS and electronic non-nicotine delivery systems [ENNDS]", as well as their "consumables", "accessories", and "heated tobacco products".
E-cigarettes are the most common form of ENDS. When used, they heat a liquid to create aerosols that are inhaled by the user. These "e-liquids" contain nicotine, a highly addictive substance found in tobacco, and other additives, flavourings and chemicals, some of which are toxic to the health of both the user and those exposed to them.
PAHO/WHO recommends that governments implement regulations in line with the provisions of the FCTC and its decisions, such as prohibiting the marketing of ENDS, including their importation, distribution or sale, as well as regulations on their use in public places, prohibiting their advertising and promotion, taxing them, and other regulations similar to those applied to tobacco products.
Tobacco kills one million people in the region of the Americas per year. While measures taken since the FCTC came into force in 2005 have reduced the percentage of smokers from 28 per cent of the total population in 2000 to 16.3 per cent in 2020, these achievements are threatened by novel tobacco and nicotine products.
Currently, 11.3 per cent of adolescents between 13 and 15 years of age in the region use tobacco, compared to the world average of 10.3 per cent.
2 years 2 months ago
Medical News, Health News Latest, Medical News Today - Medical Dialogues |
Unusual Case of Spontaneous Cerebral Air Embolism- A report
The introduction of air into cerebral venous or arterial circulation known as cerebral air embolism (CAE), and it is a rare clinical entity. CAE is commonly iatrogenic secondary to central venous catheter (CVC) placement or removal, various endoscopic procedures, or trauma or surgical scenarios.
Doctors from Medanta hospital, Gurugram report a case of spontaneous CAE in an unusual scenario.
Cerebral air embolism is an uncommon clinical entity. It may be iatrogenic secondary to central venous catheter (CVC) placement or removal, hysteroscopy, laparoscopy, endoscopy, defibrillator placement, and after hemodialysis. Apart from this, cerebral air embolism may occur as a complicating factor in several clinical settings, including thoracic, cardiovascular and neurosurgical operations, and thoracic and cranial trauma.
Neurological symptoms of air embolism include seizures, altered mental status, loss of consciousness, and hemiparesis. In some cases, patients may have sudden onset of a combination of signs and symptoms. Both arterial and venous infarcts may occur as a result of air embolism.
A unique and important property of air that differs from a solid mass embolus is its ability to travel retrograde against the direction of blood flow. This is a result of gas bubbles rising in blood because of their lower specific gravity.
Chronic otitis media is a chronic inflammation of the middle ear and mastoid cavity. Spread of infection from the ear and temporal bone causes intracranial complications. The routes of spread include direct erosion of bone, through normal communication- oval and round windows, vascular channels (thrombophlebitis, periarteriolar spaces of Virchow–Robin), and abnormal preformed pathways- congenital dehiscence and acquired dehiscence (fractures, surgical defect). Extracranial complications are usually direct sequelae of localized acute or chronic inflammation.
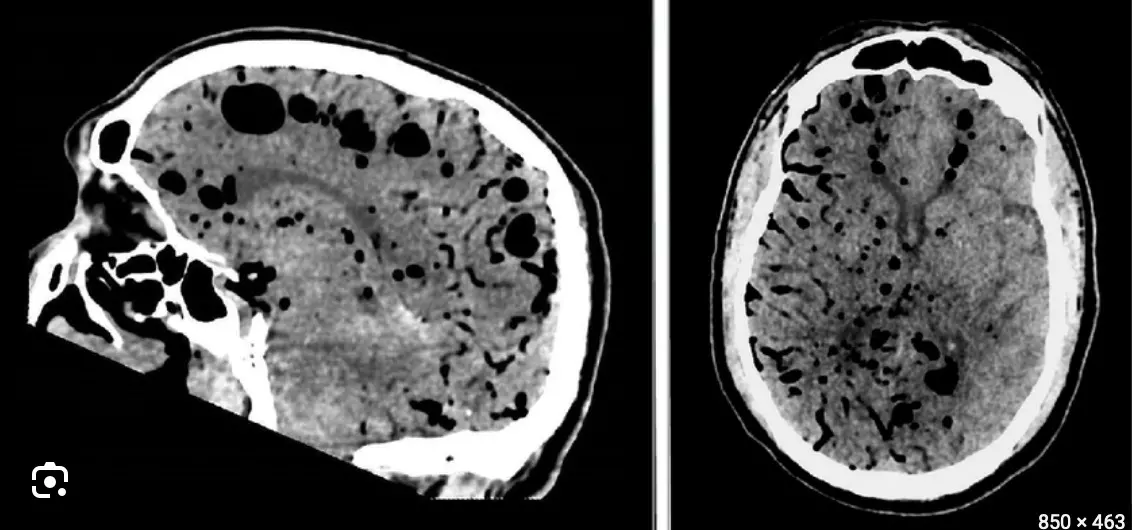
Bansal et al describe a case of a 71-year-old man who presented to emergency after developing giddiness following a yoga session which lasted for a few seconds to a minute. After the patient regained consciousness, he had confusion lasting for around 15–20 minutes following which he was able to walk on his own downstairs. The patient had complained of left ear fullness since then. He had a superficial scalp injury due to the fall. There were no associated complaints of pulsatile tinnitus, vomiting, headache, altered behavior, any focal weakness, seizures, or significant hearing loss. On examination, the patient was conscious, oriented, and alert. He did not have any focal weakness or any obvious neurological signs; only tandem walking was impaired.
His MRI brain showed marked thinning with focal erosion of the left sigmoid plate of the mastoid cavity and mastoid air cells with multiple air foci in the posterior fossa along cerebellar folia, prepontine, and suprasellar cisterns and tracking superiorly along the tentorium cerebelli likely arising from the mastoid cavity through the eroded posterior wall of the left mastoid cavity and sigmoid plate. No definite bony fracture through the mastoid or petrous temporal bone or skull base. The flow void of the transverse and sigmoid sinuses was preserved.A close possibility of hemorrhage in the left cerebellar region was kept as there was significant blooming seen on SWI imaging Thus, plain NCCT head was done which clearly revealed multiple air foci in the posterior fossa along cerebellar folia, prepontine, and suprasellar cisterns and hence the diagnosis of air embolism was established.
In view of the left sigmoid plate dehiscence, HRCT temporal bone was done which corroborated the findings of MRI brain and revealed left otitis media with mastoiditis with cerebral air embolism along bilateral cerebellar folia, prepontine, and suprasellar cisterns. His ENT examination revealed a bilateral intact tympanic membrane and normal ear, nose, and throat examination. The patient was managed conservatively with bed rest, oral antihistamines, and analgesics to which he responded very well.
The chronic otitis media causing cholesteatoma led to erosion of the left mastoid wall and the sigmoid plate. Air pressure changes during the yoga session possibly led to the leak of air into the cerebellar folia as well as prepontine and suprasellar cisterns. Thiis case highlights to consider cerebral air embolism as a differential diagnosis in such clinical scenarios.
Reference
Bansal R, Bhuyan S, Gupta R, Garg A, Bansal AR. Spontaneous Cerebral Air Embolism–An Unusual Scenario. Neurol India 2023;71:772-4
DOI: 10.4103/0028-3886.383877
2 years 2 months ago
Neurology and Neurosurgery,Top Medical News,Case of the Day,Neurology and Neurosurgery Cases
PAHO/WHO | Pan American Health Organization
Eight countries in the Americas ban electronic cigarettes
Eight countries in the Americas ban electronic cigarettes
Cristina Mitchell
25 Aug 2023
Eight countries in the Americas ban electronic cigarettes
Cristina Mitchell
25 Aug 2023
2 years 2 months ago

KFF Health News' 'What the Health?': A Not-So-Health-y GOP Debate
The Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
For the first time since 2004, it appears health insurance coverage will not be a central issue in the presidential campaign, at least judging from the first GOP candidate debate in Milwaukee Wednesday night. The eight candidates who shared the stage (not including absent front-runner Donald Trump) had major disagreements over how far to extend abortion restrictions, but there was not even a mention of the Affordable Care Act, which Republicans have tried unsuccessfully to repeal since it was passed in 2010.
Meanwhile, a new poll from KFF finds that health misinformation is not only rampant but that significant minorities of the public believe things that are false, such as that more people have died from the covid vaccine than from the covid-19 virus.
This week’s panelists are Julie Rovner of KFF Health News, Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico, Victoria Knight of Axios, and Margot Sanger-Katz of The New York Times.
Panelists
Joanne Kenen
Johns Hopkins Bloomberg School of Public Health and Politico
Victoria Knight
Axios
Margot Sanger-Katz
The New York Times
Among the takeaways from this week’s episode:
- The first Republican presidential debate of the 2024 cycle included a spirited back-and-forth about abortion, but little else about health care — and that wasn’t a surprise. During the primary, Republican presidential candidates don’t really want to talk about health insurance and health care. It’s not a high priority for their base.
- The candidates were badly split on abortion between those who feel decisions should be left to the states and those who support a national ban of some sort. Former Vice President Mike Pence took a strong position favoring a national ban. The rest revealed some public disagreement over leaving the question completely to states to decide or advancing a uniform national policy.
- Earlier this summer, Stanford University’s Hoover Institute unveiled a new, conservative, free-market health care proposal. It is the latest sign that Republicans have moved past the idea of repealing and replacing Obamacare and have shifted to trying to calibrate and adjust it to make health insurance a more market-based system. The fact that such plans are more incremental makes them seem more possible. Republicans would still like to see things like association health plans and other “consumer-directed” insurance options. Focusing on health care cost transparency could also offer an opportunity for a bipartisan moment.
- In a lawsuit filed this week in U.S. District Court in Jacksonville, two Florida families allege their Medicaid coverage was terminated by the state without proper notice or opportunity to appeal. It seems to be the first such legal case to emerge since the Medicaid “unwinding” began in April. During covid, Medicaid beneficiaries did not have to go through any kind of renewal process. That protection has now ended. So far, the result is that an estimated 5 million people have lost their coverage, many because of paperwork issues, as states reassess the eligibility of everyone on their rolls. It seems likely that more pushback like this is to come.
- A new survey released by KFF this week on medical misinformation found that the pandemic seems to have accelerated the trend of people not trusting public health and other institutions. It’s not just health care. It’s a distrust of expertise. In addition, it showed that though there are people on both ends — the extremes — there is also a muddled middle.
- Legislation in Texas that was recently signed into law by Republican Gov. Greg Abbott hasn’t gotten a lot of notice. But maybe it should, because it softens some of the state’s anti-abortion restrictions. Its focus is on care for pregnant patients; it gives doctors some leeway to provide abortion when a patient’s water breaks too early and for ectopic pregnancies; and it was drafted without including the word “abortion.” It bears notice because it may offer a path for other states that have adopted strict bans and abortion limits to follow.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week they think you should read, too:
Julie Rovner: KFF Health News’ “Doctors and Patients Try to Shame Insurers Online to Reverse Prior Authorization Denials,” by Lauren Sausser.
Margot Sanger-Katz: KFF Health News’ “Life in a Rural ‘Ambulance Desert’ Means Sometimes Help Isn’t on the Way,” by Taylor Sisk.
Joanne Kenen: The Atlantic’s “A Simple Marketing Technique Could Make America Healthier,” by Lola Butcher.
Victoria Knight: The New York Times’ “The Next Frontier for Corporate Benefits: Menopause,” by Alisha Haridasani Gupta.
Also mentioned in this week’s episode:
- NPR’s “Two Families Sue Florida for Being Kicked off Medicaid in ‘Unwinding’ Process,” by Selena Simmons-Duffin
- NPR’s “Texas Has Quietly Changed Its Abortion Law,” by Selena Simmons-Duffin.
- KFF’s “Poll: Most Americans Encounter Health Misinformation, and Most Aren’t Sure Whether It’s True or False.”
Click to open the transcript
Transcript: A Not-So-Health-y GOP Debate
[Editor’s note: This transcript, generated using transcription software, has been edited for style and clarity.]
Julie Rovner: Hello and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News. And I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, Aug. 24, at 10 a.m. As always, news happens fast, and things might have changed by the time you hear this. So, here we go. We are joined today via video conference by Margot Sanger-Katz of The New York Times.
Margot Sanger-Katz: Good morning.
Rovner: Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico.
Joanne Kenen: Hi, everybody.
Rovner: And Victoria Knight of Axios News.
Victoria Knight: Hello, everyone.
Rovner: No interview this week, but we’ll have an entire interview episode next week. More on that later. First, we will get to this week’s news. Well, Wednesday night saw the first Republican presidential debate of the 2024 cycle, minus front-runner Donald Trump, in what could only be called a melee, on Fox News Channel. And while there was a spirited debate about abortion, which we’ll get to in a minute, I didn’t hear a single word about anything else health-related — not Medicare or Medicaid, nor any mention of the Affordable Care Act. Was anybody surprised by that? For the record, I wasn’t. I wasn’t really expecting anything except abortion.
Kenen: Well, somebody, I think it was [former New Jersey Gov. Chris] Christie actually pointed out that nobody was talking about it.
Knight: Mike Pence. It was [former Vice President] Mike Pence, actually.
Kenen: Oh, Pence. OK. “Nobody’s talking about Medicare and Social Security.” And then he didn’t talk about it, and nobody mentioned the ACA.
Rovner: Is the ACA really gone as a Republican issue, for this cycle, do we think?
Kenen: Well, I think it’s become, like, a guerrilla warfare. Like, they’re still trying to undermine it. They’re not trying to repeal it, but they’re looking at its sort of soft underbelly, so to speak, and trying to figure out where they can put more market forces on, which we can sort of come back to later. But they spent 10 years trying to repeal it, and they just figured out what they’ve got to do now is pretend it’s not there. Right now, abortion is their topic.
Rovner: Well, let us turn to that.
Sanger-Katz: Yeah, I was just going to say that we’ve been seeing this happen a little bit over the last couple of cycles. In the 2020 race — I went through the transcripts of all of the speakers during the Republican National Convention and was really staggered by how few mentions of Obamacare there were relative to the way that the issue had been discussed in the past. But I think — just a note, that this is the Republican debate. Republicans don’t really want to be talking about health insurance and health care, because they don’t really have affirmative plans to put forward and because I think that they see that there are some real political liabilities in staking out a strong position on these issues. But in a general election, I think it will be impossible for them to avoid it, because, I think, Joe Biden has a lot of things that he wants to say. I think he is very committed to, in particular, broadcasting that he wants to protect Medicare. I think he’s quite proud of the expansions that he’s made of the Affordable Care Act. And so, this is a little bit of a weird moment in the race because, you know, we really only have one party that’s having a primary, and its leading candidate is not participating in the debates. And so, I think these candidates are trying to focus elsewhere. But it is — I will say, as someone who’s covered a couple of these now — it is a weird experience to have health care and health policy feel like a second-tier issue, because it was so central — Obamacare, in particular — was just so central to so many of these election cycles and such an animating and unifying issue among Republican voters, that this kind of post-failure-of “repeal and replace” era feels very different.
Kenen: One really quick thing is, they’re going to hit Biden on inflation. Economically, it’s his most vulnerable point, and health care costs are a burden. And I was a little surprised, without going into Obamacare and repeal and all that stuff, they mentioned the price of food, the price of gas, they mentioned interest rates and housing. It would have been really easy, and I expect that at some point they will start doing it, to talk about the cost of health care, because Biden’s done a huge amount on coverage and making insurance more affordable and accessible. But the cost of health care, as we all know, is still high in America.
Rovner: And at very least, the cost of prescription drugs, which has been a bipartisan issue going back many, many years. All right. Well, the one health issue that, not surprisingly, did get a lot of attention last night was abortion. With the exception of Mike Pence, who has been an anti-abortion absolutist for his entire tenure in Congress, as governor of Indiana, and as vice president, everyone else looked pretty uncomfortable trying to walk the line between the very anti-abortion base of the party and the recognition that anti-abortion absolutism has been a losing electoral strategy since the Supreme Court overturned Roe last year. What does this portend for the rest of the presidential race and for the rest of the down-ballot next year? Rather than trying to bury the fact that they all disagree, they all just publicly disagreed?
Knight: And I think they also, like, if you listened, [former U.S. ambassador to the United Nations] Nikki Haley kind of skirted around how she would address it. She talked about some other things, like contraception and saying that there just weren’t enough votes in the Senate to pass any kind of national abortion ban. [Florida Gov.] Ron DeSantis also, similarly, said he was proud of his six-week bill but didn’t quite want to answer about a national abortion ban. There were the few that did say, like, Hey, we’re into that. And some said, You know, it needs to go back to the states. So there definitely was kind of this slew of reactions on the stage, which I think just shows that the Republican Party is figuring out what message, and they don’t have a unified one on abortion, for sure.
Rovner: I do want to talk about Nikki Haley for a second, because this is what she’s been saying for a long time that she thinks that there’s a middle ground on abortion. And, you know, bless her heart. I’ve been covering this for almost 40 years and there has never been a middle ground. And she says, well, everybody should be for contraception. Well, guess what? There’s a lot of anti-abortion stalwarts who think that many forms of contraception are abortion. So there isn’t even a consensus on contraception. Might she be able to convince people that there could be a middle ground here?
Sanger-Katz: Oh, what I found sort of interesting about her answers: I think on their face they were kind of evasive. They were like, I don’t need to answer this question because there’s not a political consensus to do these things. But I do think it was sort of revealing of where the political consensus is and isn’t that I think she’s right. Like, realistically, there aren’t the votes to totally ban abortion; there aren’t the votes to renew the Roe standard. And I think she was in some ways very honestly articulating the bind that Republicans find themselves in, where they, and I think a lot of their voters, have these very strong pro-life values. At the same time, they recognize that getting into discussions about total abortion bans gives no favors politically and also isn’t going to happen in the near future. So, I felt like, as a journalist, you know, thinking about how I would feel having asked her that question, I felt very dissatisfied by her answer, because she really didn’t answer what she would like to do. But I do think she channeled the internal debate that all these candidates are facing, which is, like, is it worth it to go all the way out there with a policy that I know will alienate a lot of American voters when I know that it cannot be achieved?
Rovner: I was actually glad that she said that because I’ve been saying the opposite is true also — everybody says, well, why didn’t, you know, Congress enshrine abortion rights when they could have? The fact is, they never could have. There have never been 60 votes in the Senate for either side of this debate. That’s why they tried early after Roe to do national bans and then a constitutional amendment. They could never get enough votes. And they tried to do the Freedom of Choice Act and other abortion rights bills, and they couldn’t get those through either. And this is where I get to remind everybody, for the 11,000th time, the family planning law, the Title X, the federal Family Planning [Services and Public Research] Act, hasn’t been reauthorized since 1984 because neither side has been able to muster the votes even to do that. Sorry, Joanne, you wanted to say something.
Kenen: No, I thought Haley’s response on abortion was actually really pretty interesting on two points, right? She didn’t technically answer the question, but she also said this question is a fantasy — you know, face it. And, you know, she said that, and then she mentioned the word contraception. She did not dwell on it. She sort of said it sort of quickly. She missed an opportunity, maybe, just for one or two more sentences. You know, she said we need to make sure that contraception … she’s the only woman on that stage. She’s a mother; she’s got two kids. And, you know, there is uncertainty. After Dobbs there were advocacy groups saying, you know, they’re going to ban contraception tomorrow, and that didn’t happen. And we still don’t know how that fight will play out and what types of contraception will be debated. But I noticed that she said that on a stage full of Republicans, and I noticed that nobody else — all men — didn’t pick up on it.
Rovner: The big divide seemed to be, do you want to leave it completely to the states or do you want to have some kind of national floor of a ban? And they seemed, yeah —
Kenen: Yeah, and the moderators didn’t pick up on that. I mean, there was such a huge brouhaha on the stage. You know, the moderators had a lot of trouble moderating last night. It wouldn’t have been easy for them to get off of abortion and follow up on contraception. But I thought it was just sort of an interesting thing that she noted it.
Sanger-Katz: I will say also, and I agree with Julie: With the possible exception of Mike Pence, even the candidates that were endorsing some kind of national abortion policy, we’re talking about a 15-week gestational limit. There really wasn’t anyone who was coming out and saying, “Let’s ban all abortions. Let’s even go to six weeks,” which many of the states, including Florida, have done. So I do think, again, like, even the candidates that were more willing to take an aggressive stand on whether the federal government should get involved in this issue were moderating the position that you might have expected for them before Dobbs.
Kenen: But even 15 weeks shows how the parameters of this conversation have changed, because what the Republicans had been doing pre-Dobbs was 20 weeks, with their so-called fetal-pain bills. So 15 weeks, which would have sounded extremely radical two years ago — compared to six weeks, 15 sounds like, oh, you know, this huge opportunity for the pro-choice people. And it is another sign of how this space has shrunk.
Sanger-Katz: Yeah, no, I don’t mean that it’s a huge opportunity for the pro-choice people, but I think it reflects that even the candidates who were willing to go the most out on the limb in wanting to enforce a national abortion restriction understand the politics do not permit them to openly advocate going all the way towards a full ban.
Rovner: While we are on the subject of Republicans and health, there actually is a new Republican plan to overhaul the health system. Sort of. It’s from the Hoover Institution at Stanford, from which a lot of conservative policy proposals emanate. And it’s premised on the concept that consumers should have better control of the money spent on their health care and a better idea of what things cost. Now, this has basically been the theme of Republican health plans for as long as I can remember. And the lead author of this plan is Lanhee Chen, who worked for Republicans in the Senate and then led presidential candidate Mitt Romney’s policy shop, and whose name has been on a lot of conservative proposals. But I find this one notable more for its timing. Republicans, as we mentioned, appear to have internalized the idea that the only thing they can agree on when it comes to health care is that they don’t like the Affordable Care Act. Is that changing or is this just sort of hope from the Republican side of the policy wonk shop?
Sanger-Katz: I think this is connected to the discussion that we had about the debate, but it feels to me like we are in a bit of a post Obamacare era where the fights about “Are we going to continue to have Obamacare or not?” have sort of faded from the mainstream of the discussion. But there’s still plenty of discussion to be had about the details. The Democrats clearly want to expand Obamacare in various ways. Some of those they have done in a temporary fashion. Others are still on the wish list. And I think this feels very much like the kind of calibration adjustment, you know, small changes, tinkers on the Republican side to try to make the health insurance market a little bit more market-based. But this is not a big overhaul kind of plan. This is not a repeal-and-replace plan. This is not a plan that is changing the basic architecture of how most Americans get their insurance and how it is paid for. This is a plan that is making small changes to the regulation of insurance and to the way that the federal government finances certain types of insurance. That said, I think the fact that it’s more incremental makes it feel like these are things that are more likely to potentially happen because they feel like there are things that you could do without having a huge disruptive effect and a big political backlash and that you could maybe develop some political consensus around.
Rovner: It does, although I do feel like, you know, this is a very 2005 plan. This is the kind of thing that we would have seen 15 years ago. But as Democrats have gotten the Affordable Care Act and discovered that the details make it difficult, Republicans have actually gotten a lot on the transparency side and, you know, helping people understand what things cost. And that hasn’t worked very well either. So there’s a long way to go, I think, on both sides to actually make some of these things work. Victoria, did you want to add something?
Knight: Yeah, I’ve been talking to Republicans a lot, trying to figure out like what is their next go-to going to be. And I think they’re pretty understanding that ACA is set in place, but they still don’t want to give up that there are alternative types of health insurance that they want to put out there. And I think that seems that’s kind of what they realize they can accomplish if they get another Republican president and they’re going to try to do association health plans again. They’re going to try to expand some of these what they call health reimbursement arrangements, things like that, to just like kind of try to add some other types of health insurance options, because I think they know that ACA is just too entrenched and that there’s not much else they can do outside of that. And then, yeah, I think focus a little more on the transparency and cost because they know that’s a winning message and that is the one thing in Congress right now on the health care end that seems to have bipartisan momentum for the most part.
Rovner: Yeah, I think you’re absolutely right. Well, another issue that could have come up in last night’s debate but didn’t was the unwinding of Medicaid coverage from the pandemic. The news this week is that the first lawsuit has been filed accusing a state of mistreating Medicaid beneficiaries. The suit filed against Florida by the National Health Law Program and other groups is on behalf of two kids, one with a disability, and a mom who recently gave birth. All would seem to still be eligible, and the mom says she was never told how to contest the eligibility determination that she was no longer eligible, and that she was cut off when she tried to call and complain. State officials say their materials have been approved by the Centers for Medicare & Medicaid Services, which they have, and that Florida, in fact, has a lower procedural disenrollment rate than the average state, which is also true. But with 5 million people already having been dropped from Medicaid, I imagine we’re going to start to see a little more pushback from advocacy groups about people who are, in all likelihood, still eligible and have been wrongly dropped. I’m actually a little surprised that it took this long.
Kenen: Many of the people who have been dropped, if they’re still eligible, they can get recertified. I mean, there’s no open enrollment season for Medicaid. If you’re Medicaid-eligible, you’re Medicaid-eligible. The issue is, obviously, she didn’t understand this. It’s not being communicated well. If you show up at the hospital, they can enroll you. But people who are afraid that they aren’t covered anymore may be afraid of going to the hospital even if they need to. So there’s all sorts of bad things that happen. In some of these cases, there are simple solutions if the person walks in the door and asks for help. But there are barriers to walking in the door and asking for help.
Rovner: I was going to say one of the plaintiffs in this lawsuit is a child with a disease …
Kenen: Cystic fibrosis.
Rovner: Right. That needs expensive drugs and had not been able to get her drugs because she had been cut off of Medicaid. So there’s clearly stuff going on here. It’s probably true that Florida is better than the average state, which means that the average state is probably not doing that well at a lot of these things. And I think we’re just starting to see, you know, it’s sort of mind-numbing to say, oh, 5 million people have been separated from their health insurance. And again, we have no idea how many of those have gotten other health insurance, how many of those don’t even know and won’t know until they show up to get health care and find out they’re no longer covered. And how many people have been told they’re no longer covered but can’t figure out how to complain and get back on?
Sanger-Katz: And it’s this very extreme thing that’s happening right now. But it is, in many ways, the normal system on steroids. You know, if you’ve been covering Medicaid for any period of time, as all of us have, like, people get disenrolled all of the time from Medicaid for these administrative reasons, because of some weird hiccup in the system, they move, their income didn’t match in some database. This is a problem that a lot of states face because they have financial incentives often to drop people off of Medicaid because they have to pay a portion of the cost of providing health care. And a lot of them have rickety systems, and they’re dealing with a population that often has unstable housing or complicated lives that make it hard for them to do a lot of paperwork and respond to letters in a timely way. And so part of the way that I’ve been thinking about this unwinding is that there’s a particular thing that’s happening now, and I think there’s a lot of scrutiny on it, appropriately. And I think that there should be to make sure that the states are not cutting any corners. But I also think in some ways it’s sort of like a way of pressure-testing the normal system and reminding us of all of the people who slip through the cracks in normal times and will continue to do so after this unwinding is over. And these stories in Florida, to me, do not feel that dissimilar from the kinds of stories that I have heard from patients and advocates in states long before this happened.
Rovner: Yeah, I think you’re right. It’s just shining a light on what happens. I mean, it was the oddity that they were … states were not allowed to redetermine eligibility during the pandemic because normally states are required to redetermine eligibility at least once a year. And I think some do it twice a year. So it’s, you know, these redeterminations happen. They just don’t happen all in a huge pile the way they’re happening now. And I think that’s the concern.
Sanger-Katz: And it also, I think, really shines a light on the way that Medicaid is structured, where the Affordable Care Act simplified it quite a lot because, [for example], you’re in an expansion state and you earn less than a certain amount of money, then you can get Medicaid. But there are all of these categories of eligibility where, you know, you have to be pregnant, you have to be the parent of a child of a certain age. You have to demonstrate that you have a certain disability. And I think [it] is a reminder that this is a pretty complicated safety net, Medicaid. You know, there’s lots of things that beneficiaries have to prove to states in order to stay eligible. And there’s lots of things, honestly, you know, if states really want to make sure that they are reserving resources for the people who need them, that they do need to be checking on. And so I think we’re all just sort of seeing that this is a messy, complicated process. And I think we’re also seeing that there are these gaps and holes in who Medicaid covers. And it’s not the case that we have a perfect and seamless system of universal coverage in this country. We have this patchwork and people do fall between the cracks.
Kenen: And this is one of the most vulnerable populations, obviously. Some of the elderly are also very vulnerable, but these are people who may not speak either English or Spanish. They don’t have access to computers necessarily. I mean, we’re giving the least assistance to the population that needs the most assistance. And, you know, I mean, I think if Biden wanted to be really savvy about fixing it, he’d come out with some slogan about “Instead of Medicare unwinding, it’s time to have Medicare rewinding,” or something like that, because they’re going to have to figure … I mean, they have taken some steps, but it’s a huge mess, and the uninsurance rate is going to go up, and hospitals are going to have patients that are no longer covered, and it’s not going to be good for either the health care system or certainly the people who rely on Medicaid.
Rovner: I think it’s noteworthy how much the administration has been trying not to politicize this, that apparently, you know, we keep hearing that they won’t even tell us which states, although you can … people can sort of start to figure it out. But, you know, states that are having a more difficult time keeping eligible people on the rolls, shall we say, when the administration could have … I mean, they could be trumpeting, you know, which states are doing badly and trying to shame them. And they are rather very purposely not doing that. So I do think that there’s at least an attempt to keep this as collegial, if you will, as possible in a presidential election year. So my colleagues here at KFF have a depressing, but I guess not all that surprising, poll out this week about medical misinformation and how much of the public believes things that simply aren’t true — like that more people died from the covid vaccine than covid itself, or that ivermectin is a useful treatment for the virus. It’s not. It’s for parasites. And the survey didn’t just ask about covid. People have been exposed to, and a significant percentage believe, things like that it’s harder to get pregnant if you’ve been on birth control and stop. It isn’t. Or that people who keep guns in their house are less likely to be killed by a gun than those who don’t. They’re not. But what’s really depressing is the fact that the pandemic seems to have accelerated an already spiraling trend in distrust of public institutions in general: government, local and national media, and social media. Are we ever going to be able to start to get that back? I mean, you know, we talk about the woes with public health, but this goes a lot deeper than that, doesn’t it?
Kenen: And it’s not just health care. When you look at historical metrics about trust — which I’ve had to for a course I teach — we were never a very trusting society, it turns out. We’ve had large sectors of the population haven’t been trusting of many institutions and sectors of society for decades. We’re just not too huggy in this country. It’s gotten way worse. And what you said is right, but it’s broad. It’s not just doctors. It’s not just vaccines, it’s expertise. This distrust is really corrosive. But of all the things in that survey, one that really blew me away was we’re like, what, 13 years since Obamacare was passed? Only 7% or 8% — “only,” I should say only in quotes, you know — only 7% or 8% still thought there were death panels, but something like 70% wasn’t sure if there were death panels. Like, has anyone known anyone who went before a death panel? Since 2010? And yet 70% — I mean, I may be a little off, I didn’t write it down — but it’s something like 70% weren’t sure. And that is a mind-blowing number. It just says, you know, they weren’t ready to come out and say, yes, there are death panels. But that meant that a lot of Democrats also weren’t sure if there were death panels There are no death panels.
Knight: I was just gonna say, I also thought it was interesting that it showed people do use social media to get a lot of their information, but then they also don’t trust the information that they get on there. So it’s kind of like, yeah …
Rovner: And they’re right not to!
Knight: Yeah, they’re absolutely right not to. But then it’s also like, well, they’re then just not getting health information at all, or if they’re getting it, they just don’t trust it. So just showcasing how difficult it is to fill that void of health information, like, people just aren’t getting it or don’t trust it.
Rovner: I feel like some of this is social literacy. I mean, you know, we talk about health literacy and things that people can understand, but, you know, people don’t understand the way journalism works, the difference between the national news and what you see on Facebook. And I think that’s, Joanne, going back to your point about people not trusting expertise, it’s also not being able to figure out what expertise is and who has expertise. I mean, that’s really sort of the bottom line of all this, isn’t it?
Kenen: Well, I mean, I was doing some research — I can’t remember the exact details, this was something I read several months ago — but there was one survey maybe a couple of years ago where the majority of people said they don’t trust the news they read, but they’re still getting their news from something that they don’t trust. So it sounds sort of funny, but it’s actually not. I mean, it’s really a crisis of people don’t know what to believe. The uncertainty is corrosive, and it’s health care and politics, this widening chasm of people with alternative sets of facts — or alternative worldviews, anyway. So it’s not good. I mean, it was a really good survey, it was a really interesting survey, but some of it wasn’t so surprising. I mean, that there’s still people who, like, the fertility issues and the vaccines. You can sort of understand why those have lingered in the environment we’re in. I had actually had a conversation the other day with a political scientist who had studied the death panel rumors 10 years ago. And I said, what about now? And, you know, he was sort of … he hadn’t looked at it and he was sort of saying, well, you know, there aren’t any. And people have probably figured that out by now. Well, no. I have to email him the study, right?
Sanger-Katz: Anytime that I read a study like this, I am also reminded — and I think it is useful for all of us to be reminded of this and probably most people who are listening to the podcast — that the average American is just not as tuned in on the news and on the Washington debate and on the minutia of public policy, as all of us are. So, you know, and I think that that is part of the reason why you see so many people not sure about these things. It’s clearly the case that they are being exposed to bad information and that is contributing to their uncertainty. And I think the rise of misinformation about both health policy and about actual, you know, health care, in the case of covid, is a bad and relatively newer phenomenon. But I also think a lot of people just aren’t paying that close attention, you know, and it’s good to be reminded of that.
Kenen: The book I just read that I referred to — it’s by an MIT political scientist named Adam Berinsky, and it’s called “Political Rumors.” And it just came out, and he was talking about exactly that, that we’re all exposed to misinformation. We can’t avoid it. It’s everywhere. And that for people who aren’t as engaged with day-to-day politics, they end up uncertain. That’s this messy middle, which they also use in the KFF survey. They came up with a very similar conclusion about the “muddled middle,” I think was the phrase they used. And what this political scientist said to me the other day was that, you know, pollsters tend to not look at the “I don’t know, I’m uncertain, no opinion.” They sort of shunt them aside and they look at the “yes” or “no” people. And he was saying, no, no, no, you know, this is the population we really need to pay attention to, the “Uncertains” because they’re probably the ones you can reach more. And in the real world, we saw that with vaccination, right? I mean, in the primary series — I mean, booster takeup was low — but in the primary when there was a lot of uncertainty about the vaccines, the people who said “no way I am ever going to get the vaccine” — I mean, KFF was surveying this every month — most of them didn’t. You know, a few on the margins did, but most of them who were really militantly against the vaccine didn’t take it. The ones who were “I don’t know” and “I’m a little scared” and “I’m waiting and seeing” … a lot of them did take it. They were reached. And that’s sort of an important lesson to shift the focus as we deal with distrust, as we deal with disinformation and we deal with messaging, which is good, and truth-building and confidence-building, it is that muddled middle that’s going to have to be more of a target than we have traditionally thought.
Rovner: Well, in the interest of actually giving good information, we have a couple of updates on the reproductive health front. For those of you keeping score, abortion bans took effect this week in South Carolina and Indiana after long drawn-out court battles. Meanwhile, in Texas, an update to our continuing discussion of women with pregnancy complications who’ve been unable to get care because doctors fear running afoul of that state’s ban, a couple of weeks ago, reports Selena Simmons-Duffin at NPR, Texas Gov. Greg Abbott very quietly signed a law that created a couple of exceptions to the ban for ectopic pregnancies and premature rupture of membranes, both of which are life-threatening to the pregnant woman, but just not necessarily immediately life-threatening. I had not heard a word about this change in the law until I saw Selena’s story. Had any of you?
Kenen: In fact, it should have come up because of this court case in Texas about, you know, a broader health exception — it’s not even “health,” it’s life-threatening. It’s like, at what point do you get sick enough that your life is in danger as opposed to, you know, should you be treating that woman before … you see what direction it’s going, and you don’t let them go to the brink of death? I mean, that was the court case and Abbott fought that. But yeah, it was interesting.
Rovner: It was a really interesting story that was also, you know, pushed by a state legislator who was trying very hard not to … never to say the word abortion and to just make sure that, you know, this was about health care and not abortion. It’s an interesting story, we will link to it.
Sanger-Katz: I wonder if other states will do this as well. It seems like, as we’ve discussed, you know, abortion bans are not as popular as I think many Republican politicians thought they would [be]. And I do think that these cases of women who face really terrible health crises and are unable to get treated are contributing to the public’s dislike of these policies. And on the one hand, I think that there is a strong dislike of exceptions among people who support abortion bans because they don’t want the loopholes to get so big that the actual policy becomes meaningless. On the other hand, it seems like there is a real incentive for them in trying to fix these obvious problems, because I think it contributes to bad outcomes for women and children. And I think it also contributes to political distaste for the abortion ban itself.
Kenen: But it’s very hard to legislate every possible medical problem … I mean, what Texas did in this case was they legislated two particular medical problems. And some states … they have the ectopic — I mean, ectopic is not … there’s no stretch of the imagination that that’s viable. Right? The only thing that happens with an ectopic pregnancy is it either disintegrates or it hemorrhages. I mean, the woman is going to have a problem, but making a list of “you get this condition, you can have a medical emergency abortion, but if you have that condition and your state legislator didn’t happen to think about it, then you can’t.” I mean, the larger issue is: How do you balance the legal restrictions and medical judgments? And that’s … I don’t think any state that has a ban has completely figured that out.
Rovner: Right. And we’re back to legislators practicing medicine, which is something that I think the public does seem to find distasteful.
Sanger-Katz: I mean, I don’t think that this solves the problem at all, but I think it does show a surprising responsiveness to the particular bad outcomes that are getting the most publicity and a sort of new flexibility among the legislators who support these abortion bans. So it’s interesting.
Rovner: All right. Meanwhile, another shocking story about pregnant women being treated badly. The Centers for Disease Control and Prevention reported this week that a survey conducted this April found that 1 in 5 women reported being mistreated by medical professionals during pregnancy or delivery. For women of color, the rate was even higher: more than 1 in 4. Mistreatment included things like getting no response to calls for help, being yelled at or scolded, and feeling coerced into accepting or rejecting certain types of treatment. We know a lot of cases where women in labor or after birth reported problems that went ignored. Among the most notable, of course, was tennis legend Serena Williams, who gave birth to her second child this week after almost not surviving the birth of her first. We’re hearing so much about the high maternal mortality rate in the U.S. What is it going to take to change this? This isn’t something that can be solved by throwing more money at it. This has got to be sort of a change in culture, doesn’t it?
Kenen: No. I mean, it’s … if someone who’s just given birth, particularly if it’s the first time and you don’t know what’s normal and what’s not and what’s dangerous and what’s not dangerous, and, you know, it’s a trauma to your body. I mean, you know, I had a very much-wanted child, but labor is tough, right? I always say that evolution should have given us a zipper. But the philosophy should be, if someone who’s just been through this physical and emotional ordeal, has discomfort or a question or a fear, that you respect it and that you calm it down, you don’t dismiss it or yell at somebody. When you’re pregnant, you read all these books and you go to Lamaze workshops and you learn all this stuff about labor and delivery. You learn nothing about what happens right after. And it’s actually quite uncomfortable. And no one had ever told me what to expect. And I didn’t know. And I always, like, when younger women are having babies, I let them know that, you know, talk to your doctor or learn about this or be prepared for this, because that is a really vulnerable point. And that this survey — and it’s more Black and poor women, and Latina women in this survey, it’s not that … it’s disproportionate like everything else in health care — they’re being disrespected and not listened to. And some of them are going to have bad medical outcomes because of that.
Rovner: As we are seeing. All right. Well, that is this week’s news now. We will take a quick break. Then we will come back and do our extra credit.
Hey, “What the Health?” listeners: You already know that few things in health care are ever simple. So if you like our show, I recommend you also listen to “Tradeoffs,” a podcast that goes even deeper into our costly, complicated, and often counterintuitive health care system. Hosted by longtime health journalist and my friend Dan Gorenstein, “Tradeoffs” digs into the evidence and research data behind health care policies and tells the stories of real people impacted by decisions made in C-suites, doctors’ offices, and even Congress. Subscribe wherever you get your podcasts.
OK, we’re back. It’s time for our extra-credit segment. That’s when we each recommend a story we read this week we think you should read too. As always, don’t worry, if you missed it; we will post the links on the podcast page at KFFHealthNews.org and in our show notes on your phone or other mobile device. Victoria, why don’t you go first this week?
Knight: So my extra credit is from The New York Times, and the story is called “The Next Frontier for Corporate Benefits: Menopause.” It basically details how a lot of companies are realizing that, you know, as more women get into leadership positions, high-level leadership, executive positions, they’re in their 40s, late 40s, early 50s, that’s when menopause or perimenopause starts happening. And that’s something that can last for a while. I didn’t realize the stories, that it can last almost 10 years sometimes. And so it was talking about how, you know, it affects women for a long period of time. It can also affect their productivity in the workplace and their comfort and being able to accomplish things. And so they were realizing, you know, we kind of need to do something to help these women stay in these positions. And there was actually an interesting tidbit at the very end where it was talking about some companies may even be, like, legally compelled to make accommodations. And that’s due to the new Pregnant Workers Fairness Act, which says that employers have to provide accommodations for people experiencing pregnancy but also related medical conditions. They’re saying menopause could be included in that. And just some of the benefits some of these companies were offering were access to virtual specialists, but they were talking about, like, if they need to do other things like cooling rooms and stuff like that. So I thought it was kind of interesting. And another employer benefit that maybe some employers are thinking about adding.
Kenen: I think all offices should have, like, little nap cubicles and man-woman, pregnant-not pregnant. And, you know, just like “life is rough.” [laughter]
Knight: I agree.
Kenen: Just a little corner!
Rovner: Joanne, why don’t you go next?
Kenen: Mine is from The Atlantic. It’s by Lola Butcher. And it is “A Simple Marketing Technique Could Make America Healthier.” And it’s basically talking about how some medical practices are doing what we in the news business and the tech industry knows of as “A-B testing.” You know, a tech company may try a big button or a little button and see which one consumers like. Newsrooms change headlines— headline A, headline B and see which one draws more readers — and that hospitals and medical practices have been trying to do. In some cases, it’s text messaging two different kinds of reminders to figure out, you know … one example was the message with something like 78 characters got women to book a mammogram, but a message with 155 characters did not. Two text messages were better than one for booking children’s vaccines. So some people are very excited about this. It’s getting people to do preventive care and routine care. And some people think this is just not the problem with health care, that it’s way deeper and more systemic and that this isn’t really going to move the needle. But it was an interesting piece.
Rovner: Any little thing helps.
Kenen: Right. This was an interesting piece.
Rovner: Margot.
Sanger-Katz: I wanted to talk about an article in KFF Health News from Taylor Sisk. The headline is “Life in a Rural ‘Ambulance Desert’ Means Sometimes Help Isn’t on the Way,” and it’s a really interesting exploration of some of the challenges of ambulance care in rural areas, which is a topic that is near and dear to my heart. Because when I was a reporter in New Hampshire covering rural health care delivery, I spent the better part of a year writing about ambulance services and the challenges there. And I think this story is highlighting a real challenge for people in these communities. And I think it’s also really a reminder that the ambulance system is this weird, off-to-the-side part of our health care system that I think is often not well integrated and not well thought of. It tends to be regulated as transportation, not as health care. It tends to be provided by local governments or by contractors hired by local governments as opposed to health care institutions. It tends to have a lot of difficulty with billing a very high degree of surprise billing for its patients, and also just a real lack of health services research about best practices for how fast ambulances should arrive, what level of care they should provide to people, and on and on. And I just think that it’s good that she’s highlighted this issue. And also, I think it is a reminder to me that ambulances are probably worth a little bit more attention from reporters overall.
Rovner: Well, my story is also something that’s near and dear to my heart because I’ve been covering it for a long time. It’s from my KFF Health News colleague Lauren Sausser. It’s called “Doctors and Patients Try to Shame Insurers Online to Reverse Prior Authorization Denials.” And it is a wonderful 2023 update to a fight that Joanne and I have been covering since, what, the late 1990s. It even includes comments from Dr. Linda Peeno, who testified about inappropriate insurance company care denials to Congress in 1996. I was actually at that hearing. The twist, of course, now is that while people who were wrongly denied care at the turn of the century needed to catch the attention of a journalist or picket in front of the insurance company’s headquarters. Today, an outrage post on Instagram or TikTok or X can often get things turned around much faster. On the other hand, it’s depressing that after more than a quarter of a century, patients are still being caught in the middle of appropriateness fights between doctors and insurance companies. Maybe prior authorization will be the next surprise medical bill fight in Congress. We shall see. All right. That is our show for the week. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review; that helps other people find us, too. Special thanks, as always, to our amazing engineer, Francis Ying. Also, as always, you can email us your comments or questions. We’re at whatthehealth@kff.org. Or you can tweet me or X me or whatever. I’m @jrovner, also on Bluesky and Threads. Joanne?
Kenen: I am also on Twitter, @JoanneKenen; and I’m on Threads, @joannekenen1; and Bluesky, JoanneKenen.
Rovner: Margot.
Sanger-Katz: I’m @sangerkatz.
Rovner: Victoria.
Knight: I’m @victoriaregisk on X and Threads.
Rovner: Well, we’re going to take a week off from the news next week, but watch your feed for a special episode. We will be back with our panel after Labor Day. Until then, be healthy.
Credits
Francis Ying
Audio producer
Stephanie Stapleton
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ ‘What the Health?’ on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
2 years 2 months ago
Courts, COVID-19, Elections, Medicaid, Multimedia, States, The Health Law, Abortion, KFF, KFF Health News' 'What The Health?', Misinformation, Podcasts, Polls, Pregnancy, texas, Women's Health
The UWI leads regional dialogue on climate change and mental health
According to Ambassador Bristol, “Climate change and mental health are recognised as two of the greatest global challenges the region faces”
View the full post The UWI leads regional dialogue on climate change and mental health on NOW Grenada.
2 years 2 months ago
Business, Environment, Health, climate change on mental health, gillian bristol, lacc, latin american-caribbean centre, the university of the west indies, the uwi
PAHO/WHO | Pan American Health Organization
Update on variant of interest EG.5 and variant under surveillance BA.2.86
Update on variant of interest EG.5 and variant under surveillance BA.2.86
Cristina Mitchell
23 Aug 2023
Update on variant of interest EG.5 and variant under surveillance BA.2.86
Cristina Mitchell
23 Aug 2023
2 years 2 months ago
How to take care of your skin
VITAMINS AND minerals play a crucial role in maintaining the health and appearance of the skin. They contribute to various skin functions, including cell regeneration, collagen production, protection against environmental damage, and overall skin...
VITAMINS AND minerals play a crucial role in maintaining the health and appearance of the skin. They contribute to various skin functions, including cell regeneration, collagen production, protection against environmental damage, and overall skin...
2 years 2 months ago
For your perfect skin
BOOSTING THE quality of your diet checks a lot of boxes for your health. Weight, energy, and proper nutrition come to mind first. The health of your skin should be added to that list as nutritional skincare illuminates the natural radiance of your...
BOOSTING THE quality of your diet checks a lot of boxes for your health. Weight, energy, and proper nutrition come to mind first. The health of your skin should be added to that list as nutritional skincare illuminates the natural radiance of your...
2 years 2 months ago

COVID-19 lockdowns may have caused myopic shift in children
Mandatory online schooling and confinement during the COVID-19 pandemic may have exacerbated myopia in school-aged children in Puerto Rico, according to a review published in Optometry and Vision Science.“Online learning increased students’ time on electronics indoors and reduced their time outside during the COVID-19 pandemic quarantine,” study author Neisha M.
Rodriguez, OD, PhD, MPH, associate professor at Inter American University of Puerto Rico School of Optometry, and colleagues wrote. “The previously mentioned factors are believed to increase a child’s
2 years 2 months ago
Health – Demerara Waves Online News- Guyana
Mahdia dorm fire victim discharged from New York’s Staten Island hospital 3 months after fatal blaze
STATEN ISLAND, New York City (WABC) — It’s been three long months of surgeries, skin grafts, physical rehabilitation, and grief counseling. But Monday, three months to the day of a fatal fire that claimed the lives of 20 students in a girl’s dormitory in Guyana, the most critically burned patient will be discharged. Mariza Williams was ...
STATEN ISLAND, New York City (WABC) — It’s been three long months of surgeries, skin grafts, physical rehabilitation, and grief counseling. But Monday, three months to the day of a fatal fire that claimed the lives of 20 students in a girl’s dormitory in Guyana, the most critically burned patient will be discharged. Mariza Williams was ...
2 years 2 months ago
Health, News